Idiopathic Giant Cell Myocarditis - A Case Report
Ratheesh P T1, Priyathap2, Shirleyvasu3
1 Assistant Professor, Department of Forensic Medicine, Govt Medical College , Calicut, India.
2 Junior Resident, Department of Forensic Medicine, Govt Medical College, Calicut, India.
3 Professor and HOD, Department of Forensic Medicine, Govt Medical College, Calicut, India.
*Corresponding Author
Ratheesh P T,
Assistant Professor,
Department of Forensic Medicine,
Govt Medical College , Calicut, India.
Tel: 9495543266
E-mail: ratheeshpt1@gmail.com
Article Type: Case Report.
Received: May 08, 2015; Accepted: June 02, 2015; Published: June 11, 2015
Citation: Ratheesh P T, Priyathap, Shirleyvasu (2015). Idiopathic Giant Cell Myocarditis - A Case Report. Int J Cardiol Res. 02(2), 25-27. doi: dx.doi.org/10.19070/2470-4563-150006
Copyright: Ratheesh P T© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited..
Abstract
Sudden cardiac death is an unexpected death from cardiac causes; early after the symptom onset or even without any symptoms [1]. This case report is on a non-atherosclerotic cause of sudden cardiac death. An young adult collapsed and died while at work. Autopsy was done in view of an unnatural death and ruling out various unnatural causes. Post mortem revealed morphological evidence of cardiac disease. On further evaluation it turned out to be a distinctive form of myocarditis. Myocarditis is the inflammation of heart which results in myocardial injury. The case report aims at discussion on clinical presentation, gross and histological findings of idiopathic giant cells myocarditis.. This case report highlights one such case, where reporting rare entities get mandated in the light of clear cut histological diagnosis after ruling out other causes of sudden death.
2.Introduction
3.Case Report
4.Discussion
5.Conclusions
6.References
KeyWords
Sudden Death; Idiopathic Giant Cell Myocarditis; Young Adult.
Introduction
Idiopathic giant cell myocarditis is a disease relatively young, predominantly healthy adults. It is one of the causes of sudden death in young adults, who are not previously known to have any heart disease or symptoms related to cardio vascular system. Saltykow was the first to describe Idiopathic giant cell myocarditis in a 37-year-old man who died suddenly after surgical drainage of an abscess [2]. Dozens of case reports and a few small series have been documented since then. The terminology of this as Fiedler’s myocarditis where pathology is spared of endocardium and pericardium. The term interstitial myocarditis is less appropriate as it is specifically the disease of myocardium. Giant cell myocarditis, the most lethal form, which is characterized by rapid deterioration, the prognosis is less favorable than in other forms of myocarditis. Idiopathic giant cell myocarditis is a usually fatal disorder that generally affects the young otherwise healthy individuals, although a minority of cases occur in association with autoimmune disorders or thymoma. Cases were described at autopsy from 1905 until 1987, and survival was generally less than 3 months from symptom onset and patients survived for one year or more with immunosuppressive support after endocardial biopsy diagnosis of idiopathic giant cell myocarditis [3]. Goldberg has reported one case in a newborn [4]. In 1993, Ren et al. described prolonged transplant-free survival in 3 patients with IGCM [5]. However the chance of having a minimal finding at autopsy nevertheless excludes the rare disease conditions like idiopathic giant cell myocarditis. In the late 1980s and 1990s, the average time from the start of symptoms to death or transplantation was only five months in GCM. However, many patients died before their name could be placed on a transplant list.
Case Report
A 27 year old male, manual labourer collapsed while at work on one morning. He was immediately taken to the near by hospital which was the Medical College Hospital and death was declared from there. The interval between the onset of symptoms and death was 25 minutes. He had no significant past medical or surgical history. There were no remarkable illnesses in the family including sudden deaths. At autopsy external examination revealed no injuries, urtricaria, rash. There were no free fluid or air in the plueral cavities and no internal hemorrhages. Stomach content showed no unusual appearance or smell. Mucosa appeared normal. Heart weighed 420 grams and appeared enlarged. Epicardium over left ventricle showed odema and erythema .There were multiple petechial hemorrhages over the epicardium. Endocardium was whitish in colour and cut surface showed multiple fibroticarea and inflamed hemmorhagic areas (Figure 1.1). There were areas of normal endocardium intermingled with in the fibrotic areas. Left ventricle wall measured 2cm and right ventricle wall measured 0.6cm. The lungs were odematous. All internal organs intact and were unremarkable. The entire heart was subjected to histological examination.
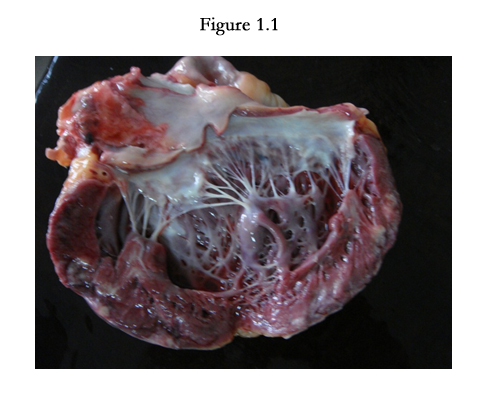

Figure 1.1
The hematoxylin and eosin stain of bits from the left ventricle showed inflammatory infiltrate predominated by lymphocytes and multinucleated giant cells without a tuberculoid or sarcoid picture (Figure 2.1-2.2)
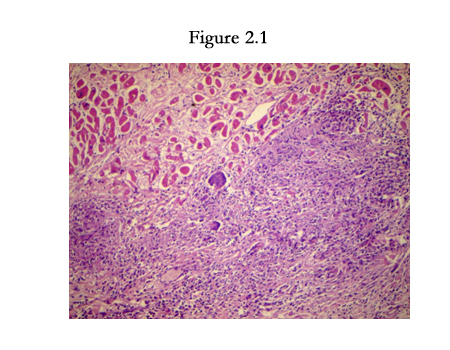
Figure 2.1
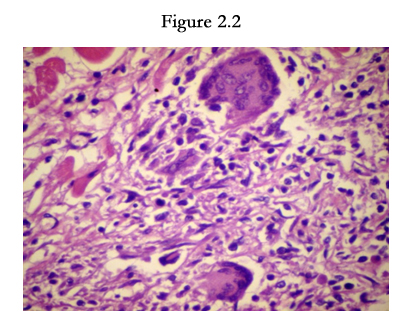
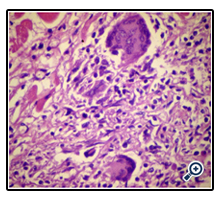
Figure 2.2
Discussion
Sudden death is defined as the sudden or unexpected termination of life of apparently healthy individuals from natural diseases. The World health organization defines sudden death as death within 24 hours from the onset of symptoms [6]. Emphasis is made on the unexpected character rather than the suddenness of the death.
Idiopathic giant cell myocarditis has an unknown etiology and hence the name. It is a rare but frequently fatal form of myocarditis, in previously healthy adults. It is usually fatal without treatment, and may respond to aggressive medical and surgical therapy and is most often progressive over days to weeks and frequently requires the concurrent management for congestive cardiac failure, tachyarrhythmias or heart block. After common causes of heart disease are excluded, the diagnosis must be confirmed by endomyocardial biopsy. No sex predominance have been mentioned in the literature and no age group is spared of this fatal condition. In infants and children epidemics have been reported. The common mode of presentation includes 1). Sudden death 2). Unexplained progressive heart failure 3). Persistant disturbance of rhythm. There are however many cases in the literature where sudden death is the first and last episode of a clinical story suggestive of myocarditis [7]. Death occurs in weeks or months unless aggressive immunosuppression or cardiac transplant is observed [8].
On gross examination, confluent and multifocal areas of necrosis are easily observed in the heart. The heart weight is normal or increased slightly. All chambers of heart are involved in most cases. The ventricular wall appears thin in those late or healed stages of the disease. Though endocardial and pericardial involvement can occur, myocardium is primarily centered. Microscopically regions of composed of widespread or multifocal serpiginous necrosis with mixed inflammatory infiltrate including lymphocytes and histiocytes were considered diagnostic. The presence of eosinophils were noted in most cases. Admixed with the infiltrate were multinucleated giant cells in the absence of sarcoid-like granuloma [9]. Immunohistochemistry studies show a macrophage/monocyte origin of the giant cells because they stain with CD68 and not with muscle markers like actin, desmin and myoglobin[10].Giant cells are evidence of inflammation and provide proof of myocarditis, the process may be acute or sub acute with repair and granulation tissue formation. The differential diagnosis of giant cells are true granuloma, tuberulous like formation and epitheloid cells. It may be seen in scar tissues of healed wounds. The overlap with sarcoidosis is difficult to distinguish, which may be explained with the unknown etiology of both the entities. However the close attention to the discriminating factor is the presence or absence of granuloma. Myocyte necrosis of broad zonal distribution is the feature of idiopathic giant cell myocarditis whereas sarcoidosis shows a mass like effect [11].
Conclusion
Of all the reasons into consideration of a sudden death, the portal of entry of death was identified to be the heart from the gross findings and confirmed by the histological study. In this particular case establishing a cause of death through ruling out all the unnatural causes. Ancillary tests were undertaken including Microbiological, Virology studies, chemical examination on blood and viscera to rule out poisoning, which all were unrewarding. The findings in the heart well pointed at a myocarditis which was found to be a very distinctive form in the histological survey. The features mentioned in the literature was a total fit in in this case as the sudden of an young adult, who was previously normal. The diagnosis of idiopathic giant cell myocarditis was first of its kind in the autopsy specimen, hence reporting such a case will be an eye opener to the cases of sudden death in young adults.
I express my sincere gratitude to Dr. Shirley Vasu, Prof & HOD for her guidance and immense support with the case and to Dr. K Prasannan for the valuable suggestions given on this paper and also to the Post graduates and faculties of the Department of Forensic Medicine. I would like to extend my gratitude to the Department of Pathology, Govt.Medical College, Kozhikode for the beautiful slides.
References
- Aaronaes M, Haugaa KH, Andreassen AK et al., (2005) Giant cell myoacraditis- a rare but dangerous disease.Tidsskrift for den Norske Laegeforening 125(16): 2198-2201.
- Saltykow S (1905) Ueber diffuse Myokarditis. Virchows Arch PatholAnat-Berl 182:1-39.
- Menghini VV, Savcenko V, Olson LJ, Tazelaar HD, Dec GW et.al (1999) Combined immune suppression for the treatment of idiopathic giant cell myocarditis. Mayo ClinProc. 74: 1221–1226.
- Goldberg GM (1955) Myocarditis of giant-cell type in an infant. Am J Clin Pathol.25: 510–513.
- Ren H, Poston RS Jr, Hruban RH, Baumgartner WA, Baughman KL, et.al., (1993) Long survival with giant cell myocarditis. Modern Pathology 6(4): 402–407.
- World Health Organization (1985) Sudden Cardiac death report of a WHO Scientific group. WHO Tech Rep Ser 726: 5-25.
- Helwig FC, Wilhelmy EW (1939) Sudden and unexpected death from acute interstitial myocarditis : A report of three cases. Ann Int Med 13(1):107-114.
- Cooper LT Jr, Berry GJ, Shabetai R (1977) Idiopathic giant cell myocarditis: natural history and treatment. Multicenter giant cell Investigators. NEngl J Med 336: 1860-1866.
- Davies MJ, Pomerance A, Teare RD (1975) Idiopathic giant cell myocarditis - a distinctive clinico-pathological entity. Br Heart J 37(2): 192-195.
- Ariza A, Lopez MD, Mate JL, et.al., (1995) Giant cell myocarditis: monocytic immune type of giant cells in case associated with ulcerative colitis, Hum Pathol 26:121-123.
- Okura Y, Dec GW, Hare JM, Kodama M, Berry GJ, et.al., (2003) A clinical and histopathological comparison of cardiac sarcoidosis and idiopathic giant cell myocarditis.J Am CollCardiol 41(2): 322-329.





