A Rare Case of Situs Inversus with Mesocardia
Sajith J S*, Gobbur R H, Koti P, Patil S V
Department of Pediatrics, Shri B M Patil Medical College and Research Center, Bijapur, India.
*Corresponding Author
Sajith J S,
Department of Pediatrics,
Shri B M Patil Medical College and Research Center,
Bijapur, India.
Tel: 919008818402
E-mail: sajithjs@yahoo.co.in
Article Type: Case Report.
Accepted: March 22, 2014; Published: March 25, 2014
Citation: Sajith J S, Gobbur R H, Koti P, Patil S V (2014) A Rare Case of Situs Inversus with Mesocardia. Int J Cardiol Res. 1(1), 1-3. doi: dx.doi.org/10.19070/2470-4563-140001
Copyright: © 2014 Sajith J S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
A ten year old male child having congenital heart disease admitted with recurrent history of respiratory infection. ECHO cardioraphy showed Mesocardia, congenitally corrected TGA, bidirectional VSD and severe pulmonary valve stenosis.On sonographic evaluation showed intra-abdominal mirror imaging of all the solid organs and vessels which was suggestive of a rare presentation of Sinus inverses with Mesocardia. Corrective surgery as pulmonary valve balloon dilation or valvuloplasty and vestricular septal repair has to be done to the child for better morbidity and reducing the mortality risk. This anomaly complicates the diagnosis and management of acute abdominal conditions like appendicitis, diverticulitis and biliary colic.
2.Introduction
3.Case Report
4.Conclusion
5.References
KeyWords
Situs Inversus; Mesocardia; Congenitally Corrected TGA.
Introduction
Situs Inversus is a condition which affects all major structures within the thorax and abdomen. Generally, the organs are simply transposed through the sagittal plane. If the heart is shifted to the right side of the thorax along with mirror imaging of intra abdominal organs, it is known as situs inversus totalis (1 in 10,000 of the general population) and the associated anatomical and functional defects are less. If the heart remains on the normal left side of the thorax, a much rarer condition (1 in 22,000), it is known as situs inversus incompletes, and there will be multiple cardiac defects associated with this condition. The chromosomal or embryological defect that causes Situs inversus is not know but it is considered as an autosomal recessive genetic condition, which can be X-linked.
Case Report
A four year old male child born out of a non consanguineous marriage was admitted for evaluation of recurrent episodes of respiratory infections and dyspnea on exertion. Child was a known case of congenital heart disease diagnosed in the first month of life and no further follow up study was done. There was no history of cyanosis or pedal edema. No history of developmental delay and child was immunized up to the age. On admission the patient had upper respiratory infection, stable vital signs. On cardiovascular system examination apex beat palpated on 5th intercostal space 1cm medial to left midclavicular line. Pansystolic murmur heard on tricuspid area and ejection systolic murmur heard on aortic and mitral areas. On abdominal examination abnormal liver dullness and Traubs space dullness was found and child was evaluated with abdominal ultrasonography, which showed intra-abdominal mirror imaging of all the solid organs and vessels. This finding was followed by chest X-ray which showed centrally placed heart and prominent pulmonary artery and infiltrates. ECG showed sinus tachycardia with right axis deviation and abnormal wave pattern in all leads. Clinically child became stable in two days and echocardiography was done for the child who showed Mesocardia with congenitally corrected transposition of great arteries, bidirectional VSD and severe valvular pulmonary stenosis. Child was discharged with oral digoxin and potassium supplementation. Patents were advised to have monthly follow up and corrective surgery for the child.
Total Count : 15870 cells/cu mm
Neutrophil : 40 %
Lymphocyte : 52 %
Monocytes : 05 %
Eosinophils : 03 %
Haemoglobin :13.6 gms%, PCV : 40.9 % MCV-74fl,MCH -24.7 Pg, MCHC- 33.3%
Platelet Count : 3.39 lakhs /cu mm
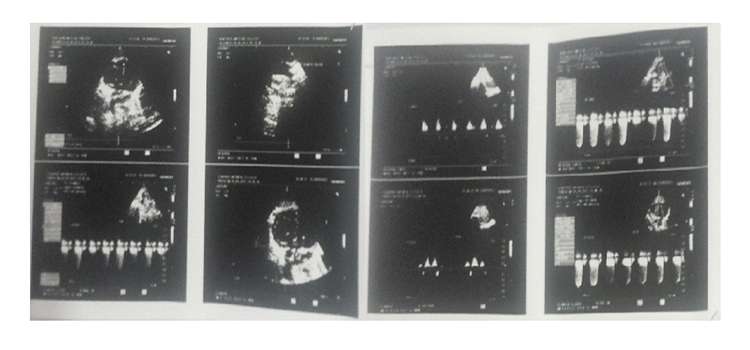

Echocardiography and Colour Doppler Report.
CHD- Situs Inverses d-loop Ventricle, Mesocardia
Congenitally corrected Transposition of Great Arteries
LA RVAorta
RALVPulmonary artery
Doubly Committed VSD (1.1 cm) with Bidirectional shunt
Severe Valvular Pulmonary Stenosis with gradient of 92 mmHg
No PDA. No coarctation of aorta
RA/LV dilated
Good biventricular function
Right aortic arch
Situs Inversus Totalis
No abnormalities detected in abdominal organs
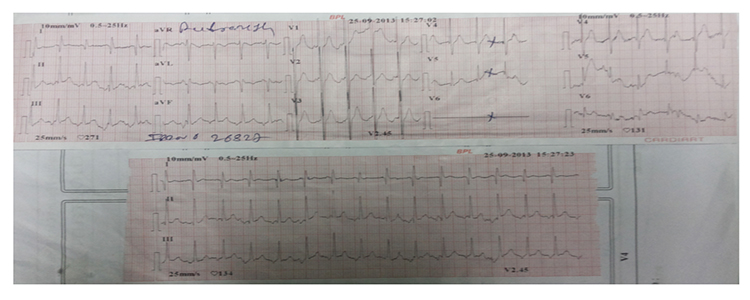

Electro Cardiography Report.
Heart rate: 136/ min
Rhythm : sinus rhythm
Right axis deviation
PR interval- 0.16 sec RR interval- 0.48 sec QRS interval- 0.08 sec
P wave- 0.08 sec Q wave-0.08 sec
R wave progression present
Biphasic P wave in lead one, aVR and V6
Tall R wave in lead one and two
Conclusion
It is an extremely rare condition to have Mesocardia in a patient with Situs Inversus. This case gives an account that mesocardia can present with multiple cardiac defects similar to situs inversus incompletes.
References
- CARDELL BS. Corrected transposition of the great vessels. Br Heart J. 1956 Apr;18(2):186–192. [PMC free article] [PubMed]
- ANDERSON RC, LILLEHEI CW, LESTER RG. Corrected transposition of the great vessels of the heart: a review of 17 cases. Pediatrics. 1957 Oct;20(4):626–646. [PubMed]
- BECK W, SCHRIRE V, VOGELPOEL L, NELLEN M, SWANEPOEL A. Corrected transposition of the great vessels. Br Heart J. 1961 Sep;23:497–511. [PMC free article] [PubMed]
- ELLIS K, MORGAN BC, BLUMENTHAL S, ANDERSEN DH. Congenitally corrected transposition of the great vessels. Radiology. 1962 Jul;79:35–50. [PubMed]
- MORGAN J, PITMAN R, GOODWIN JF, STEINER RE, HOLLMAN A. Anomalies of the aorta and pulmonary arteries complicating ventricular septal defect. Br Heart J. 1962 May;24:279–292. [PMC free article] [PubMed]
- SHAHER RM. THE SYNDROMES OF CORRECTED TRANSPOSITION OF THE GREAT VESSELS. Br Heart J. 1963 Jul;25:431–440. [PMC free article] [PubMed]
- BERRY WB, ROBERTS WC, MORROW AG, BRAUNWALD E. CORRECTED TRANSPOSITION OF THE AORTA AND PULMONARY TRUNK: CLINICAL, HEMODYNAMIC AND PATHOLOGIC FINDINGS. Am J Med. 1964 Jan;36:35–53. [Pub- Med]
- ROTEM CE, HULTGREN HN. CORRECTED TRANSPOSITION OF THE GREAT VESSELS WITHOUT ASSOCIATED DEFECTS. Am Heart J. 1965 Sep;70:305–318. [PubMed]
- Friedberg DZ, Nadas AS. Clinical profile of patients with congenital corrected transposition of the great arteries. A study of 60 cases. N Engl J Med. 1970 May 7;282(19):1053–1059. [PubMed]
- Allwork SP, Bentall HH, Becker AE, Cameron H, Gerlis LM, Wilkinson JL, Anderson RH. Congenitally corrected transposition of the great arteries: morphologic study of 32 cases. Am J Cardiol. 1976 Dec;38(7):910–923. [PubMed]
- DE LA CRUZ MV, ANSELMI G, CISNEROS F, REINHOLD M, PORTILLO B, ESPINO-VELA J. An embryologic explanation for the corrected transposition of the great vessels: additional description of the main anatomic features of this malformation and its varieties. Am Heart J. 1959 Jan;57(1):104–117. [PubMed]
- GRANT RP. THE MORPHOGENESIS OF CORRECTED TRANSPOSITION AND OTHER ANOMALIES OF CARDIAC POLARITY. Circulation. 1964 Jan;29:71–83. [PubMed]
- Van Praagh R. What is congenitally corrected transposition? N Engl J Med. 1970 May 7;282(19):1097–1098. [PubMed]
- PLATZER W. Zwei Fälle von Transpositionen mit funktioneller Korrektur. Virchows Arch. 1955;327(4):400–418. [PubMed]
- LEV M, ROWLATT UF. The pathologic anatomy of mixed levocardia.A review of thirteen cases of atrial or ventricular inversion with or without corrected transposition. Am J Cardiol. 1961 Aug;8:216–263. [PubMed]
- ROSENBAUM HD, PELLEGRINO ED, TRECIOKAS LJ. Acyanotic levocardia. Circulation. 1962 Jul;26:60–72. [PubMed]
- VANPRAAGH R, VANPRAAGH S, VLAD P, KEITH JD. ANATOMIC TYPES OF CONGENITAL DEXTROCARDIA: DIAGNOSTIC AND EMBRYOLOGIC IMPLICATIONS. Am J Cardiol. 1964 Apr;13:510–531. [PubMed]
- Lev M, Liberthson RR, Golden JG, Eckner FA, Arcilla RA. The pathologic anatomy of mesocardia. Am J Cardiol. 1971 Oct;28(4):428–435. [PubMed]
- Dick M, 2nd, Van Praagh R, Rudd M, Folkerth T, Castaneda AR. Electrophysiologic delineation of the specialized atrioventricular conduction system in two patients with corrected transposition of the great arteries in situs inversus (I,D,D). Circulation. 1977 Jun;55(6):896–900. [PubMed]
- Attie F, Soni J, Ovseyevitz J, Muñoz-Castellanos L, Testelli MR, Buendia A. Angiographic studies of atrioventricular discordance. Circulation. 1980 Aug;62(2):407–415. [PubMed]
- Graham TP, Jr, Jarmakani JM, Atwood GF, Canent RV., Jr Right ventricular volume determinations in children. Normal values and observations with volume or pressure overload. Circulation. 1973 Jan;47(1):144–153. [PubMed].





