Validation Trial of a Novel Marker of Delayed Chemotherapy-induced Emesis
Higa GM1,2*, Auber ML2, Hobbs G2
1 School of Pharmacy, Morgantown, WV, USA.
2 School of Medicine, Morgantown, WV, USA.
*Corresponding Author
Gerald M. Higa, Pharm D,
Professor of Clinical Pharmacy,
Clinical Professor of Medicine, Schools of Pharmacy and Medicine,
Robert C. Byrd Health Sciences Center, PO Box 9520, West Virginia University
26506-9520, USA.
Tel: 304-293-1461
E-mail: ghiga@hsc.wvu.edu
Received: September 02, 2016; Accepted: October 17, 2016; Published: October 19, 2016
Citation: Higa GM, Auber ML, Hobbs G (2016) Validation Trial of a Novel Marker of Delayed Chemotherapy-induced Emesis. Int J Cancer Stud Res. 5(4), 106-110. doi: dx.doi.org/10.19070/2167-9118-1600020
Copyright: Higa GM© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Post hoc analyses of study data suggested that the ratio of substance P to 5-HIAA/creatinine was a novel marker associated with risk of developing delayed chemotherapy-induced emesis. In order to verify this finding, a new clinical trial was conducted to prospectively evaluate the marker in patients receiving chemotherapy of high emetic risk level. Treatment in this study was restricted to two doxorubicin and cyclophosphamide-containing regimens. Prior to chemotherapy, blood and urine samples were collected. Serum substance P and urine 5-HIAA and creatinine (Cr) were measured to calculate patient-specific ratios. The attending oncologist had the option to follow current antiemetic guidelines or the investigators’ recommendation based on the subject’s pretreatment marker ratio.Delayed chemotherapy-induced emesis was the primary symptom monitored.Calculated ratios were ranked highest to lowest using the previously identified value of >70 as the cutoff. Of the 36 patients enrolled in the study, 11 had ratios associated with increased risk of delayed emesis. Mean pretreatment ratios for patients with (+) and without (-) emesis were 74.2 and 48.8, respectively. Although non-parametric analysis indicated the between-emesis group variance was not significantly different, p=0.154, a clear trend was observed with a higher percentage of subjects exhibiting delayed symptoms with ratios >70.
2.Introduction
3.Patients and Methods
3.1.Patient Eligibility was Based on the Following Criteria
3.2.Study Design
3.3.Neurotransmitter Measurement
3.4.Data analysis
4.Results
5.Discussion
6.Conclusion
7.Financial & Competing Interest Disclosure
8.Informed Consent Disclosure
9.References
Keywords
5-HIAA; Creatinine; Delayed Emesis; Serotonin; Substance P.
Introduction
Cancer statistics indicate that patient survival has increased over the past three decades [1]. This improvement is most frequently attributed to the development of novel therapeutic agents and conduct of well-conceived clinical trials. Less often (or not even) mentioned as a contributor to survivorship is the impact supportive care measures may have had in reducing cancerrelated morbidity and possibly, even mortality [2, 3]. However, the principal factor associated with these accomplishments may ultimately be the improved understanding of complex genomic, molecular, and biochemical pathways that regulate cancer processes and treatment-related adverse effects. While the latter conclusion may be invariably correct, there is a striking anomaly associated with one facet of supportive care, the prophylaxis of chemotherapy-induced emesis (CiE). Frequently considered as one of the most important areas of advances made in clinical oncology, CiE continues to be among the most concerning side effects patients associate with cancer therapy [4].
In spite of the clinical efficacy of antagonists that block the 5-hydroxytryptamine 3, (5-HT3) and neurokinin-1 (NK1) receptor signaling pathways, classification of anticancer agents based on emetogenic risk level, identification of patient-related risk factors, and promotion of rational antiemetic guidelines, fulfillment of the frequently espoused goal of preventing emesis, especially delayed symptoms, has been far from absolute.
Based on data initially identifying a threshold ratio (i.e., >70) of substance P (sP) to 5-hydroxyindole acetic acid (5- HIAA)/creatinine (Cr) that appeared to be associated with development of delayed CiE among patients receiving a variety of chemotherapy regimens, we subsequently extended upon our previous findings in a uniform cohort of patients [5, 6]. These studies provided the rationale for conducting a validation trial to prospectively test the predictive value of these neurotransmitters in patients undergoing doxorubicin and cyclophosphamide-based chemotherapy treatment. The aim of this paper is to report our findings related tothe association between this novel marker and risk of delayed CiE.
Patients and Methods
The clinical research study received full approval of the Institutional Review Board of West Virginia University. Complete details of the methods associated with this research study have been reported previously [5]. As such, only a brief recapitulation of the study methods is presented here.
- diagnosis of breast cancer or non-Hodgkin’s lymphoma (NHL),
- treatment with doxorubicin and cyclophosphamidecontaining chemotherapy regimens; either “AC” for breast cancer or “CHOP” + rituximab for NHL,
- performance status: 0 to 1 by Eastern Cooperative Oncology Group standards,
- absence of baseline vomiting (or nausea), and
- signed informed consent form.
Patients who met the above criteria were eligible to participate in this clinical study. None of the subjects were taking antibiotics or opiate analgesics at study entry or during the study-observation period. Identification of these potential confounding factors enabled the study to focus on chemotherapy as the principal contributing cause of emesis if symptoms developed. Blood and urine were collected in a single instancebefore chemotherapyin order to calculate patient-specific ratios of the neurotransmitters.
The major reason for inclusion of patients with two different diagnoses was related to a notable discrepancy between the two doxorubicin and cyclophosphamide-containing chemotherapy regimens. Despite relatively similar doses of both drugs, only the “AC” regimen is considered high-emetic risk level. Even though triple drug (i.e., NK1 and 5-HT3 receptor antagonists plus dexamethasone) prophylaxis is recommended for patients receiving “AC”, the attending oncologist had the option to use a two drug regimen (i.e., minus the NK1 receptor antagonist) for CiE prophylaxis based on the results of the pretreatment neurotransmitter ratio. Similarly, while routine antiemetic prophylaxis for the cohort of patients with NHL included only dual (5-HT3 receptor antagonist and dexamethasone) therapy, the attending oncologist had the option to utilize the threedrug regimen if the neurotransmitter ratio suggested otherwise. Of note, regardless of whether two or three drugs were used antiemetic prophylaxis consisted of only one dose of each agent. Administration of chemotherapy began at approximately 1100 hours in all patients. Specific information related to number (and timing) of emetic episodes (as well as grading of nausea) was obtained from all subjects through completion of self-assessment diaries. Delayed emesis in this study was defined as >2 episodes occurring after the first 24 hours (up to 120 hours) following initiation of chemotherapy. Although delayed vomiting may begin earlier than this arbitrarily determined time, 24 hours has been most frequently used to define the separation between acute and delayed symptoms [7].
Approximately 3mLs of peripheral blood was collected in serum separator tubes. In order to stabilize the protein, 500 KIU/mL of aprotonin was added to the blood samples within five minutes of collection. The blood was allowed to clot, then centrifuged at 1000 x G for 10 minutes at 4C. Serum was removed and diluted 1:2 with the kit assay buffer. Substance P was measured using a commercially available immunoassay (Substance P Assay, ParameterTM, Catalog Number KGE007, R & D Systems, Inc. Minneapolis, MN). The assay is based on the competitive binding technique in which SP present in a sample competes with a fixed amount of horseradish peroxidase-labeled sP for sites on a mouse monoclonal antibody. In brief, during incubation the monoclonal antibody becomes bound to the goat anti-mouse antibody coated onto the microplate. Following a wash to remove excess conjugate and unbound sample, a substrate solution is added to the wells to determine the bound enzyme activity. The color development is stopped and the absorbance is read at 450 nm (uQuantTM, Bio-Tek Instruments, Winooski, VT). The intensity of the color is inversely proportional to the concentration of SP in the sample. All samples were tested in duplicate as recommended by the manufacturer.
Because 5-HIAA is the major serotonin metabolite, the breakdown product was determined to be a reliable surrogate of the neurotransmitter. After adjusting the pH of the urine specimen with hydrochloric acid, the appointed metabolite and creatinine were quantitatively assayed by high-performance liquid chromatography (HPLC).
Absolute values of sP and 5-HIAA/Cr were determined for each patient. As stated in our previous reports, the possibility of neurotransmitter overlap (i.e., involvement of both neurotransmitters) in the genesis of delayed emesis provided a strong rationale for evaluating values of both neurotransmitters simultaneously. As such, the ratio of sP to 5-HIAA/Cr was selected because clinical trials assessing the efficacy of 5-HT3 and NK1 receptor antagonists suggested sP had a relatively greater role in the delayed phase compared to serotonin [8, 9].
sP to 5-HIAA/Cr ratios were arranged numerically, highest to lowest (Table 1); corresponding information related to development of delayed emesis is also noted for each of the ratio values. Between-emesis group variance (log[mean]) for each of the pre-specified markers of patients who did (+) or did not (-) develop delayed emesis was analyzed by One way ANOVA, JMPTM, Version 12.0.1, SAS Institute, Cary, NC.
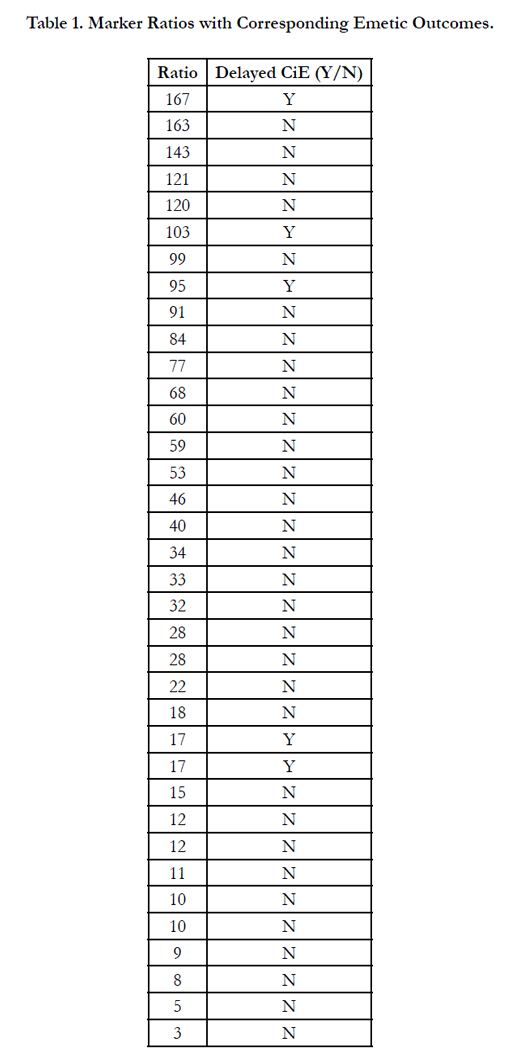

Table 1. Marker Ratios with Corresponding Emetic Outcomes.
Results
Between March 2014 and February 2016, 36 patients provided signed informed consent to participate in the study; demographics of the study population are shown in Table 2. Among the entire cohort of subjects enrolled in the study, delayed emesis developed in only five subjects, all of who received triple-drug antiemetic prophylaxis. Three of these five patients had sP to 5-HIAA/ Cr ratio of >70. Mean values of the pretreatment variables for patients with (+) and without (-) emesis were 74.2 and 48.8, respectively. Non-parametric analysis indicated the betweenemesis group variance was not significantly different, p=0.154. None of the patients with non-Hodgkin’s lymphoma developed delayed CiE. Although the primary endpoint was delayed emesis, moderate to severe nausea was reported in 21 patients, all with diagnoses of breast cancer; two subjects (both males) with NHL reported mild nausea only.
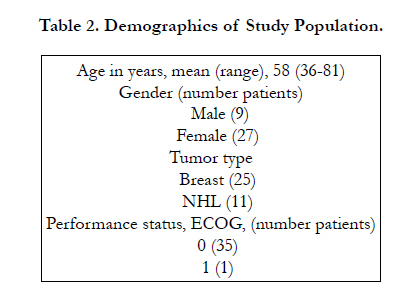
Table 2. Demographics of Study Population.
Discussion
Results of clinical trials suggest that serotonin and substance P play prominent roles in acute and delayed CiE, respectively [8-10]. These findings are potentially important especially with regard to the use of NK1 receptor antagonists (RA). Recently, post hoc analysis of data indicated the risk of developing delayed emesis was associated with a marker, the ratio of sP to 5-HIAA/Cr >70 [5, 6]. In order to prospectively determine the predictive value of this marker, an IRB-approved clinical trial was conducted involving subjects who may receive the NK1RA, aprepitant, as antiemetic prophylaxis.
A critical analysis of the data in patients who were treated with two doxorubicin and cyclophosphamide-containing chemotherapy regimens did not validate the premise that the pretreatment ratio of sP to 5-HIAA/Cr >70 was associated with risk of developing delayed CiE. However, embedded within the data are two issues of note. One relates to the small number of subjects (i.e. 11) with ratios greater than 70. Of the nine patients with breast cancer who received the three-drug prophylaxis, three developed delayed emesis. That six of the nine patients had no emetic episodes is consistent with previous reports of the overall efficacy associated with addition of an NK1 RA to the antiemetic regimen [11, 12]. The second relates to the larger cohort of subjects with ratios <70. Even though the predicted incidence of delayed emesis in this set of patients would be lower, the use of the NK1 RA in 16 subjects treated with “AC” may have masked what would have been a higher rate of emetic events had the agent not been used (as was recommended by the study investigators) based on the ratio alone. Using the same rationale described previously in subjects with ratios >70 and based on the high emetogenic risk level associated with this chemotherapy regimen, it was estimated that no more than 11 patients with breast cancer would have truly benefitted from the addition of the NK1RA suggesting that the other five subjects would not have required the same drug for a comparable outcome. Indeed, this belief is supported by two clinical trials in patients with breast cancer undergoing “AC” treatment [13, 14]. With this supposition, a significant probability of developing delayed emesis for those above the threshold ratio (compared to subjects with ratios below the cutoff) was found by Fisher’s Exact Test, p=0.0372.
Perhaps the most important piece of information gained from this study was an explanation why the CHOP regimen is not also classified as high emetic risk. Despite relatively similar doses of doxorubicin and cyclophosphamide and foregoing use of an NK1 RA, none of the subjects with NHL developed delayed emetic symptoms; and only two (male) patients reported nausea, which was rated as mild in both cases. These outcomes strongly suggest prophylaxis for delayed-phase symptoms was partially (or even in large part) attributable to multi-day prednisone therapy in the CHOP regimen, the dosage of which was approximately two-fold higher than the dose of dexamethasone used in most clinical trials [11, 14].
The relevance of these findings in daily clinical practice could be minimized by a number of salient issues. First, and foremost,the results of the ratio’s predictive value did not reach statistical significance. However, inherent also in the data was a clear trend for developing delayed emesis among subjects with ratios >70 compared to those with ratios less than that value, 27% and 8%, respectively. Second, the only statistically significant finding resulted from data speculated upon. Nonetheless, construction of the two groups (i.e., with and without emesis) was based on insight from larger clinical studies which evaluated two-andthree- drug prophylaxis in similar patients [11, 12]. Third, there is a notable imbalance in numbers of patients with breast cancer compared to NHL. However, it was reassuring that the clinical efficacy of adding an NK1 RA to patients treated with “AC” and a high ratio was consistent with results from previously published studies [11, 12]. Furthermore, the finding that only two of 16 patients with breast cancer and ratios below 70 had delayed emesis suggests that a smaller, yet significant, subset of patients undergoing “AC” treatment would do well with only 5-HT3 RA and dexamethasone prophylaxis. Fourth, consistent adherence to antiemetic guidelines precluded the use the baseline ratios in a truly prospective manner. Nevertheless, the findings reconfirm the efficacy of glucocorticoids as prophylaxis for delayed emesis and support the conclusion that the precise biochemical mechanisms for delayed symptom development is not exclusively mediated by substance P [15].
Conclusion
Current recommendations for prevention of delayed CiE are based almost exclusively on chemotherapy emetic-risk level. Arguably, “AC”, which is classified as high-emetic risk, is one of the few treatment regimens that consider both gender and clinical experience. That similar dosages of doxorubicin and cyclophosphamide in the “CHOP” regimen do not garner the same emetic risk classification partially supports the previous statement. Furthermore, clinical experience with the two drug combination (i.e.,”A” and “C”) in patients with NHL appears to justify a moderate-risk classification, one that is likely attributable to multi-day doses of high-dose glucocorticoid.
These data represent the final phase of our study related toa novel marker associated with risk of delayed emetic symptoms. We were not able to prospectively validate the marker’s predictive value, in part, because the relatively small sample size may have been insufficient to show statistical significance.
Financial & Competing Interest Disclosure
The clinical trial from which the data originated as well as the final data analysis was conducted using residual funds of one of the investigators (GMH). As such, no financial or material support was received specifically for completion of this research study; all of the data remain the property of the authors. No other financial relationship exists between any entity and any of the authors.
Informed Consent Disclosure
The authors obtained verbal and signed informed consent from every patient who participated in the clinical study.
References
- Siegel RL, Miller KD, Jemal A (2016) Cancer statistics, 2016. CA: Cancer J Clin. 66(1): 7-30.
- Wang J, Zhao Z, Barber B, Sherrill B, Peeters M, et al., (2011) A Q-TWiST analysis comparing panitumumab plus best supportive care (BSC) with BSC alone in patients with wild-type KRAS metastatic colorectal cancer. Br J Cancer. 104(12): 1848-1853.
- Ahmed N, Ahmedzai S, Vora V, Hillam S, Paz S (2004) Supportive care for patients with gastrointestinal cancer. Cochrane Database Syst Rev. 3: CD003445.
- Grunberg SM, Deuson RR, Mavros P, Geling O, Hansen M, et al., (2004) Incidence of chemotherapy-induced nausea and emesis after modern antiemetics. Cancer.; 100(10): 2261-2268.
- Higa GM, Auber ML, Hobbs G (2012) Identification of a novel marker associated with risk for delayed chemotherapy-induced vomiting. Support Care Cancer. 20(11): 2803-2809.
- Higa GM, Cumpston A, Auber ML, Hobbs G (2014) Further evidence of an association between the ratio of substance P to 5-HIAA/Cr and delayed chemotherapy-induced vomiting. Cancer Clin Res.
- Kris MG, Gralla RJ, Tyson LB, Clark RA, Cirrincione C, Groshen S (1989) Controlling delayed vomiting: double-blind, randomized trial comparing placebo, dexamethasone alone, and metoclopramide plus dexamethasone in patients receiving cisplatin. J ClinOncol. 7(1): 108-114.
- Hesketh PJ, Grunberg SM, Gralla RJ, Warr DG, Roila F, et al., (2003) The oral neurokinin-1 antagonist aprepitant for the prevention of chemotherapyinduced nausea and vomiting: a multinational, randomized, double-blind, placebo-controlled trial in patients receiving high-dose cisplatin--the Aprepitant Protocol 052 Study Group. J ClinOncol. 21: 4112-4119.
- Van Belle S, Lichinitser MR, Navari RM, Garin AM, Decramer Ml, et al., (2002) Prevention of cisplatin-induced acute and delayed emesis by the selective neurokinin-1 antagonists, L-758298 and MK-0869. Cancer. 94: 3032-3041.
- Cubeddu LX (1996) Serotonin mechanisms in chemotherapy-induced emesis in cancer patients. Oncology. 53(1): 18-25.
- Roila F, Ruggeri B, Ballatori E, Del Favero A, Tonato M (2014) Aprepitant versus dexamethasone for preventing chemotherapy-induced delayed emesis in patients with breast cancer: a randomized double-blind study. J Clin Oncol. 32(2): 101-106.
- Warr DG, Hesketh PJ, Gralla RJ, Huss HB, Herrstedt J, et al., (2005) Efficacy and tolerability of aprepitant for the prevention of chemotherapy-induced nausea and vomiting in patients with breast cancer after moderately emetogenic chemotherapy. J ClinOncol. 23: 2822-2830.
- Aapro M, Fabi A, Bole F, Medici M, Steger G, et al., (2010) Double-blind, randomized, controlled study of the efficacy and tolerability of palonosetron plus dexamethasone for 1 day with or without dexamethasone on days 2 and 3 in the prevention of nausea and vomiting induced by moderately emetogenic chemotherapy. Ann Oncol. 21: 1083-1088.
- Aapro MS, Rugo H, Rossi G, Rizzi G, Borronini Me, et al., (2014) A randomized phase III study evaluating the efficacy and safety of NEPA, a fixed-dose combination of netupitant and palonosetron, for the prevention of chemotherapy-induced nauseas and vomiting following moderately emetogenic chemotherapy. Ann Oncol. 25: 1328-1333.
- Higa GM, Auber ML, Altaha R, Kurian S, Hobbs G (2009) Concordance between substance P levels and antiemetic guidelines. J SuppOncol. 7(4): 138-142.





