Are there any Dermoscopic Signs of Primary Cutaneous Follicular Center B-cell Lymphoma?
K.Moustaide1*, S.Gallouj, Aqil Niema, FZ. Mernissi
Dermatology Venerology hospital hassan II Fes, Morocco.
*Corresponding Author
Kaoutar Moustaide,
Dermatology, Venereology,
University Hospital Hassan II, Fes, Morocco.
Tel: 00212641796117
E-mail: kmoustaide@gmail.com
Received: February 11, 2016; Accepted: February 24, 2016; Published: February 29, 2016
Citation: K.Moustaide, S.Gallouj, Aqil Niema, FZ. Mernissi (2016) Are there any Dermoscopic Signs of Primary Cutaneous Follicular Center B-cell Lymphoma?. Int J Cancer Stud Res.5(1), 93-95.doi: dx.doi.org/10.19070/2167-9118-1600016.
Copyright: K.Moustaide© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Cutaneous follicular center B-cell lymphoma is an indolent tumor that arise on head or neck. Histology by immunotyping with monoclonal antibodies in frozen or paraffin - embedded tissue is necessary for diagnosis. The tumor is usually treated by surgery or radiotherapy, although other treatments may be used such as interferon-α, chemotherapy, and biological agents. We report the case of a 70-year-old woman C, having a son followed in our department for Primary cutaneous follicular center B-Cell lymphoma who consulted for erythematous tumour in the temporal region that exhibit special features in dermoscopy and who was diagnosed with cutaneous follicular center B-cell lymphoma after biopsy, laboratory tests, thoracic-abdominal-pelvic computed tomography and abdominal ultrasound. These observation provide a first indication that early stage PCFCCL exhibits a characteristic dermoscopic pattern which is different. Prospective studies with long term follow-up are needed to determine the value of these dermoscopic.
2.Introduction
3.Case Report
4.Discussion
5.Conclusion
6.References
Keywords
Primary Cutaneous Follicular Center B-cell Lymphoma; Dermoscopy; Hereditary.
Introduction
We report a primary cutaneous follicular center cell lymphoma (PCFCCL) with its dermoscopy that arose on face of a 70-yearold
women who has a son followed for PCFCCL.
This case is unusual because PCFCCL rarely arises on the face, and to the best of our knowledge the hereditary character and the dermoscopy of PCFCCL has so far been published in the English literature.
Case Report
A 70 year old women with a family history of a son followed in our hospital for histological proven follicular B Cell lymphoma, who underwent surgical resection with good evolution, presented with a two months history of a growing mass on the right parietal region.
Physical examination revealed a well-demarcated erythematous 4*3 cm tumor with hard- elastic consistency, non pulsatile and indolent extending in the temporal region (Figure 1).
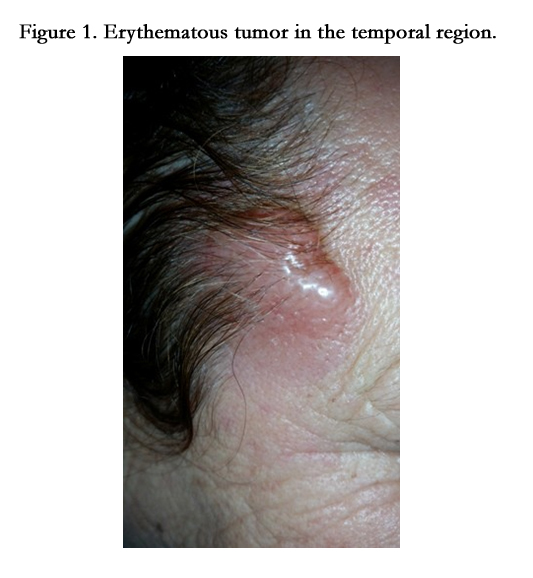

Figure 1. Erythematous tumor in the temporal region.
No lymphadenopathy, abdominal masses, or organomegaly were detected.
In front of this clinical presentation we thought about many diagnosis such us PCFCCL, Extranodal NK cell lymphoma, Merkel Carcinoma, Melanoma, Darier disease, Sarcoidosis, Pseudolymphoma, Adnexal tumor? and a Foreign body granuloma.
Dermoscopy of the tumor showed fine short linear vessel, curved linear vessel in a spermatozoa-like arrangement and purpuric spots based on an erythematous background (Figure 2).
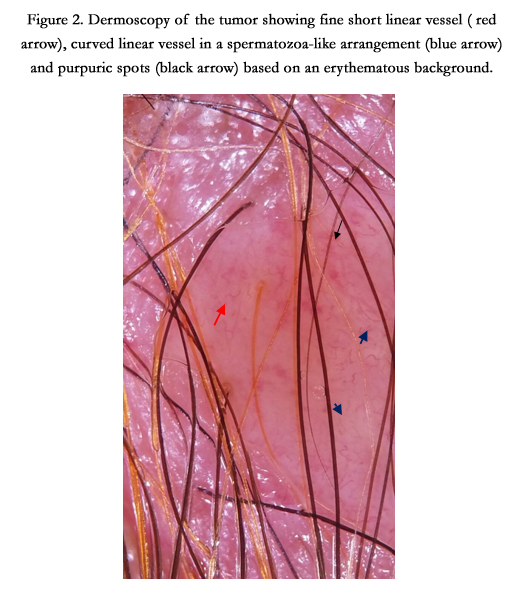
Figure 2. Dermoscopy of the tumor showing fine short linear vessel ( red arrow), curved linear vessel in a spermatozoa-like arrangement (blue arrow) and purpuric spots (black arrow) based on an erythematous background.
Histology showed a diffuse dermal infiltrate of small lymphocytes mixed with large centrocytic/entroblastic cells, partially arranged in germinal centers (Figure 3).
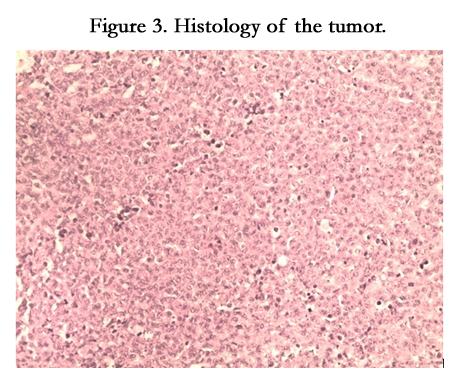
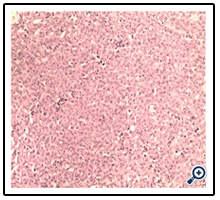
Figure 3. Histology of the tumor.
Immunohistochemistry revealed positivity of the large lymphoid cell for CD20, and negativity for CD10, CD3 ,CD5, and CD23. There was a low and very focal expression of Bcl-2 which did not express kappa or lambda chains.Moreover, neoplastic B cells showed both a high proliferation rate (MIB-1/Ki-67) and expression of nuclear Bcl-6 positivity (figure4).
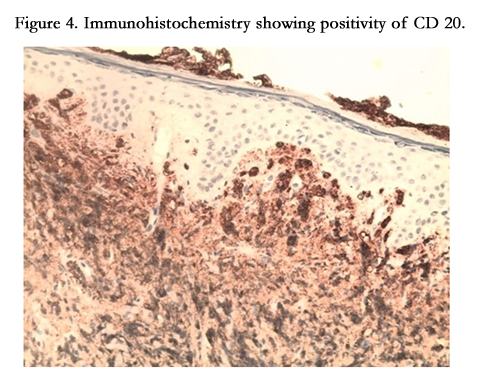
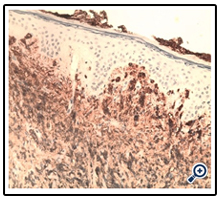
Figure 4. Immunohistochemistry showing positivity of CD 20.
A diagnosis of cutaneous primitive follicular B cell lymphoma was made.
Laboratory tests were within normal ranges. CT scan of the neck, chest, abdomen, and pelvis showed no lymphadenopathy, hepatomegaly, or splenomegaly.
The patient was scheduled for surgical resection
Discussion
Primary cutaneous B-cell lymphomas comprise approximately 20% of cutaneous lymphomas. These lymphomas typically occur on the head or neck of adults with a median age of 60 years and have a slight male predominance [1].
Few risk factors that promote the occurrence of these lymphomas have been identified. Among these factors, HIV infection, EBV, HTLV or HHV, exposure to toxic. Questions also exist about a hereditary factor [2].
While PCFCCL as defined by the EORTC has been determined to generally lackbcl-2 protein expression and the t(14;18) characteristic of nodal lymphoma, in North America they find that these features in a significant minority of PCFL. Although this discrepancy may be caused by different diagnostic criteria, it maybe that European cases of PFCL also lack bcl-2 protein and thet(14;18). Is there truly a difference in molecular pathogenesis between PCFL in North America and in Europe and how about Africa? [3].
Cutaneous follicular center B-cell lymphoma is an indolent tumor composed of neoplastic follicular center cells comprising a mixture of centrocytes (small or large, cleaved) and a variable number of centroblasts (large,noncleaved and with a prominent nucleolus). Its growth pattern may be diffuse, follicular, or mixed, and it mainly affects the back and head, although it can appear at other sites, or even at several sites without the prognosis being necessarily worse [4].
PCFCCLs are usually diffuse and neoplastic cells show cytomorphology of small and large cleaved centrocytes with centroblasts not in a cohesive sheet. Immunohistochemistry in PCFCCL shows positivity for B-cell markers CD20, CD22, CD79a, and Bcl-6 positivity and negativity for CD10, CD5, kappa, lambda, and Bcl-2 protein [3].
Therefore this case of PCFCCL appears to be unusual because it seems to have a hereditary component; however, other studies are needed to confirm this hypothesis.
Our case also indicate that PCFCCL exhibits a characteristic dermoscopic pattern consisting of fine short linear vessels and, vascular structures resembling spermatozoa which was described in early stage of mycosis fungoides and never in PCFCCL [5]. However, prospective studies with long term follow-up are needed to determine the value of these dermoscopic criteria .
PCFCCL rarely disseminates to extracutaneous sites and does not require an aggressive therapy.
Current treatment of cutaneous B-cell lymphoma involves surgical resection and/or radiotherapy, intralesional or systemic interferon alfa, chemotherapy, or rituximab.
Surgical resection is a good option in the case of an isolated lesion or a small number of lesions grouped together in one area, and it can be combined with radiotherapy.
Radiotherapy is effective against the lesions caused by primary cutaneous B-cell lymphoma and doses generally range from 20 Gy to 30 Gy. Treatment is well tolerated, and several authors consider it the first choice for localized lesions.
Interferon alfa has immunomodulatory and antitumor properties and is used less commonly in cutaneous B-cell lymphoma than in cutaneous T-cell lymphoma. The standard dose ranges from 3 to 9 million units subcutaneously per week. Interferon alfa can also be administered intralesionally.
Chemotherapy is not the treatment of choice for cutaneous B-cell lymphoma and is reserved for the more aggressive forms, such as large-cell lymphoma, leg type. The CHOP regimen (cyclophosphamide, doxorubicin, vincristine, and prednisone) is the most widely used.
Rituximab is a chimeric monoclonal anti-CD20 antibody. CD20 is a membrane phosphoprotein expressed only in B lymphocytes and is present in 95% of B-cell lymphomas. Since 1997, rituximab has been used in the treatment of non-Hodgkin B-cell lymphoma and has proven effective in cutaneous B-cell lymphoma. It can be administered intravenously or intralesionally [4].
PCFCCL have in general good prognosis with a median 5-year survival that exceeds 95 percent. 100 [6].
Conclusion
Our observation raises the genetic theory that needs to be confirmed by genomic studies on a large sample.
The dermoscopic features that we found also can help us for the diagnosis of lymphoma in our daily practice, therefore, studies comparing dermoscopic criteria of different types of lymphoma are necessary to make the diagnosis of PCFCCL easily.
References
- Zackheim HS, Vonderheid EC, Ramsay DL, LeBoit PE, Rothfleisch J, et al. (2000) Relative frequency of various forms of primary cutaneous lymphomas. J Am Acad Dermatol 43(5 Pt 1): 793-796.
- Grufferman S (2013) Epidemiology and hereditary aspects of Hodgkin and Non-Hodgkin lymphomas. In Neoplastic Diseases of the Blood. Springer, New York. 41: 849-865.
- Hsi ED (2004) Pathology of Primary Cutaneous B-Cell Lymphomas: diagnosis and classification. Clinical Lymphoma 5(2): 89-97.
- Gamo R, Calzado L, Pinedo F, López-Estebaranz JL (2008) Cutaneous Follicular Center B-Cell Lymphoma Treated with intralesional Rituximab. Actas Dermosifiliogr 99(4): 291-296.
- Lallas A, Apalla Z, Lefaki I, Tzellos T, Karatolias A, et al. (2012) Dermoscopy of early stage mycosis fungoides. J Eur Acad Dermatol Venereol 27(5): 617-621.
- Grange F, d’Incan, Vergier B (2013) Lymphomes B cutanés centrofolliculaires. Springer, Paris. 169-175.





