Implication of Pollen Sensitivity Among Patients Suffering From Chronic Urticaria – Current Scenario
R Balaji1*, BG Parasuramalu2, BC Sharath Kumar3
1* 9 Rue du Morvan, CHU Brabois Nancy, Service de Pneumologie, Bat. Specialites Medicales, 54511 Vandoeuvreles- Nancy, France.
*Corresponding Author
Dr. R Balaji,
Assistant Professor,
Department of Community Medicine,
SRM Medical College and Research Centre,
Kattankulathur,
Chennai, India.
Tel: +91 – 9790765215
E-mail: arbee2002@gmail.com
Article Type: Reserch Article
Received: July 04, 3013; Accepted: August 19, 2013; Published: September 10, 2013
Citation: R Balaji, BG Parasuramalu, BC Sharath Kumar (2013) Implication of Pollen Sensitivity Among Patients Suffering From Chronic Urticaria– Current Scenario. Int J Clin Med Allergy. 1(1), 3-7. doi: dx.doi.org/10.19070/2332-2799-130002
Copyright: R Balaji© 2013. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Studies have implicated house dust mites and foods sensitivity in chronic urticaria based on skin prick testing and in vitro analysis. Hence we wanted to study the implication of pollen sensitivity in chronic urticaria patients along with foods and dust mite allergens using Skin Prick Test method.
Methods: This study was conducted in Allergy clinic, Preventive medicine unit, Kempegowda Institute of Medical Sciences Hospital, Bangalore from January 2005 to March 2010. Totally 300 patients with confirmed clinical diagnosis of Chronic urticaria were recruited and were subjected for Skin prick test with 123 allergen extracts and the results wereanalysed and interpreted.
Results: Out of 300 chronic urticaria patients, 171(57%) were in the age group of 20–39 years. 146(48.67%) were males and 154(51.33%) were females. 181(60.33%) were having only chronic urticaria. 140(46.67%) of urticaria patients were having symptoms from 6 weeks to one year. 44(14.67%) had a family history of atopy. Majority of urticaria patients (with or without co-morbid conditions), 164(54.66%) were sensitive to food allergens followed by pollens 92(30.66%), dust mites 60(20%) and others. Among food allergens, majority 15(5%) were sensitive to masoor dal followed by almonds 14(4.66%), ginger 13(4.33%) and yeast 13(4.33%). Among pollens, majority 32(10.66%) were sensitive to Prosopis juliflora followed by Parthenium hysterophorus 17(5.66%), Peltophorum pterocarpum 17(5.66%) and Chenopodium album 16(5.33%). Among dust mites, 42(14%) and 39(13%) were sensitive to D.farinae & D.pteronyssinus respectively.
Conclusion: Pollens sensitivity is also implicated in Chronic urticaria patients along with foods and dust mite allergens.
2.Introduction
3.Materials and Methods
3.1 Procedure of skin prick testing (SPT)
4.Results
5.Discussion
6.References
Keywords
Chronic Urticaria; Skin Prick Test; Pollen Sensitivity.
Introduction
Chronic urticaria is one of the perplexing problems faced by the clinicians. Chronic urticaria is defined as daily or almost daily occurrence of urticarial wheals for at least six weeks [1]. Numerous physical agents can trigger the onset of urticaria, such as cold, heat, the sun, vibrations, rubbing (dermographism) or pressure. Urticaria can also be caused by drugs, food, infection (viral, bacterial, parasitic or fungal), insect stings, more rarely due to pneumoallergens [2,3]. Rhinitis and Asthma are other atopic diseases also affected by the above allergens [4]. Urticaria is a common disorder that affects as many as 20% of all people at sometime during their lives. The pathogenesis is complex and not well known [5]. Studies [6-9] implicated house dust mites and foods sensitivity in chronic urticaria based on skin prick testing and in vitro analysis. Hence, we wanted to study the implication/role of pollen sensitivity in patients with chronic urticaria along with foods and dust mite allergens using Skin Prick Test method which is the gold standard to diagnose the clinical sensitivity.
Materials and Methods
After obtaining the Institutional Ethical Committee approval, the present study was conducted in the Allergy clinic, Preventive medicine unit, Kempegowda Institute of Medical Sciences Hospital & Research Centre, Bangalore from January 2005 to March 2010. Totally 300 patients with confirmed clinical diagnosis of Chronic urticaria (with a duration of more than 6 weeks), with co-morbid conditions like Allergic rhinitis (ARIA guidelines)[10], Bronchial asthma (GINA guidelines) [11] and Allergic conjunctivitis who attended the Allergy clinic were recruited for the study after obtaining the informed consent. In all cases, questions regarding food allergies, drug intake, signs of infection, causes of physical urticaria, insect bites and personal and family history of atopy were asked. The clinical characteristics of the disease, such as duration, frequency and associated angioedema and symptoms of anaphylaxis were also investigated. Routine investigations such as complete blood count and urine examination were done to rule out the focus of infection. The complete history was obtained and physical examination was done to rule out the systemic diseases. The patients who were subjected to skin prick testing were instructed to stop drugs like antihistamines, bronchodilators, beta-blockers and theophylline. Skin prick tests were performed on 300 patients with 123 allergen extracts. The extracts included 19 pollens, 5 dusts, 2 dust mites, 10 fungi, 10 insects, 3 epithelia and 74 food allergens. Allergen extracts for skin prick tests were obtained
from Creative Drug Industries, Navi Mumbai.
SPT was performed on the flexor side of upper arm and forearm after cleaning with isopropyl alcohol. A single drop of each allergen extract of 1:10 concentration was placed along with positive control (Histamine) and negative control (saline).
Sterile lancet was used to prick by making a shallow lift (at an acute angle) for a second to allow adequate entry of antigen beneath the stratum corneum epidermis. This was repeated for each allergen after wiping the lancet with dry cotton. The allergen was left in place for 20 minutes then the reading of wheal area (allergen), saline area and histamine area diameter was taken with the help of measuring scale [12, 13]. Interpretation of test results was done according to Agarwal criteria [14]. Allergens, which produced wheal areas more than 2+ (grade 2 and above) were considered as positives.
Results
Out of 300 chronic urticaria patients, the maximum i.e. 171 (57%) were in the age group of 20–39 years. Among them, 146 (48.67%) were males and 154 (51.33%) were females. Among males, maximum i.e. 49 (33.56%) were in the age group of 20 – 29 years, whereas in females, maximum i.e. 43 (27.92%) were in the age group of 30 – 39 years. The mean age of chronic urticaria patients was 35.15 ± 12.96 years and the range was 8 – 72 years. (Table 1).
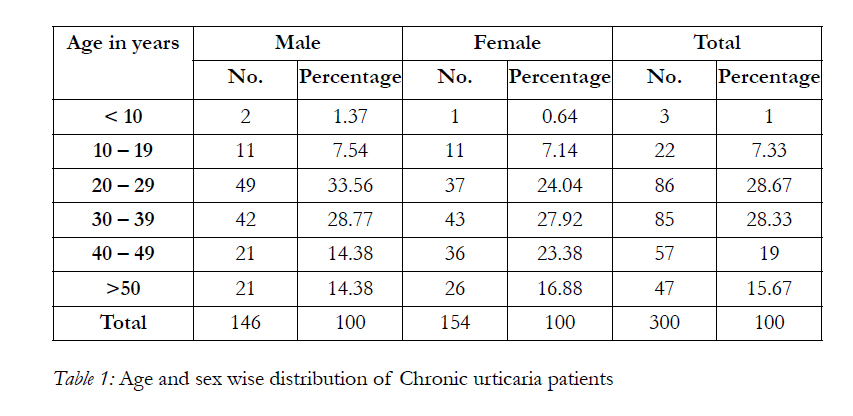

Table 1: Age and sex wise distribution of Chronic urticaria patients.
Majority i.e., 181 (60.33%) were having chronic urticaria alone. The other co-morbid conditions associated with chronic urticaria were chronic urticaria with conjunctivitis among 43 (14.33%) patients followed by chronic urticaria with allergic rhinitis among 34 (11.33%) and chronic urticaria with conjunctivitis & rhinitis among 21 (7%). (Table 2).
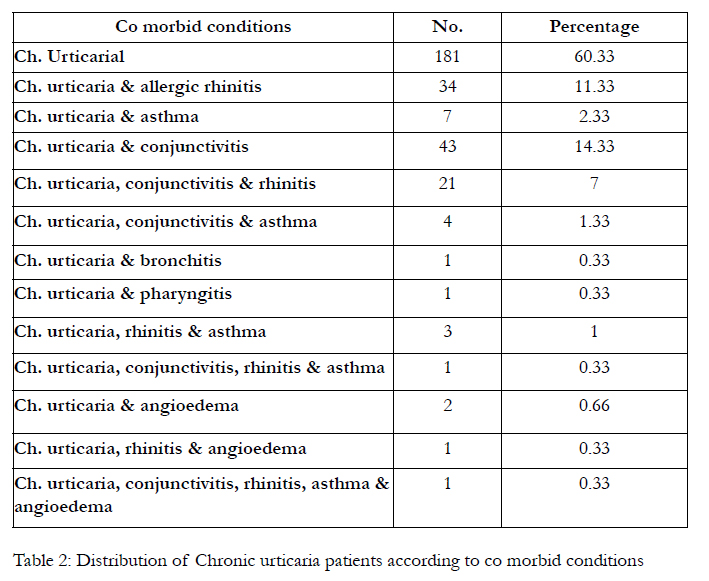
Table 2: Distribution of Chronic urticaria patients according to co morbid conditions.
The average duration of chronic urticaria was 3.3±4.2 years. Majority i.e. 140 (46.67%) patients were having symptoms from 6 weeks to one year, next highest, 49 (16.33%) were having symptoms from 5 to 10 years and the least 13 (4.33%) were having symptoms from 13 to 18 months.
Forty four (14.67%) chronic urticaria patients had a family history of atopy. Among them, 19(43.18%) had family history of atopy in mother, followed by 17(38.64%) in siblings, 8(18.18%) in father, 3(6.81%) in paternal side and 2(4.54%) in maternal side.
Majority of chronic urticaria patients (with or without co-morbid conditions) i.e., 164 (54.66%) were sensitive to food allergens, followed by pollens 92 (30.66%), dust mites 60 (20%) and others. In this study, those patients with h/o angioedema (4) were not positive for any of the allergen. (Table 3A).
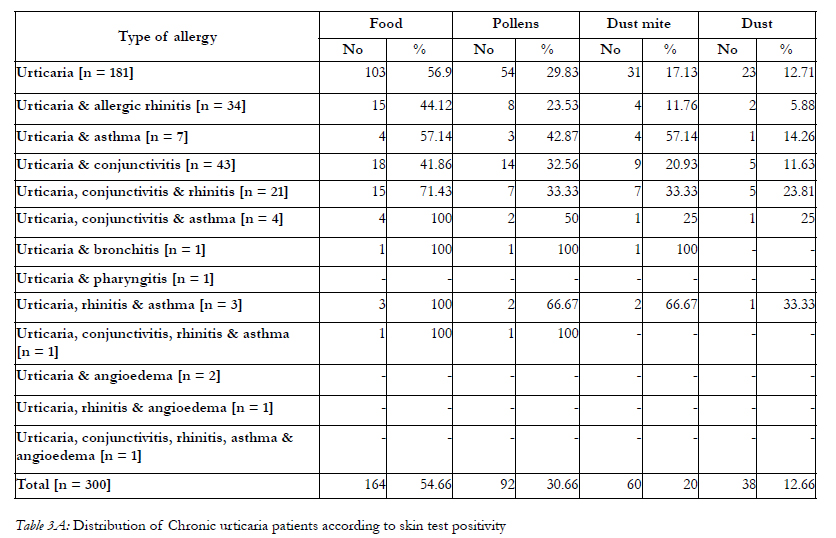
Table 3A: Distribution of Chronic urticaria patients according to skin test positivity.
The sensitivity for pollen allergens is found to be more than dust mite allergens in chronic urticarial patients (with or without co-morbid conditions) and the difference is found to be statistically significant. (Table 3B).
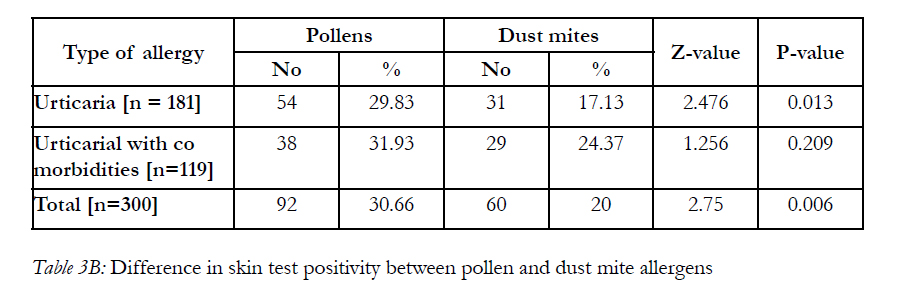
Table 3B: Difference in skin test positivity between pollen and dust mite allergens.
Among food allergens, majority of patients i.e., 15(5%) were sensitive to masoor dal, followed by almonds 14(4.66%), ginger 13(4.33%), yeast 13(4.33%) and others. (Table 4A) Among pollens, majority i.e., 32(10.66%) were sensitive to Prosopis juliflora, followed by Parthenium hysterophorus 17(5.66%), Peltophorum pterocarpum 17(5.66%), Chenopodium album 16(5.33%) and others. (Table 4B)
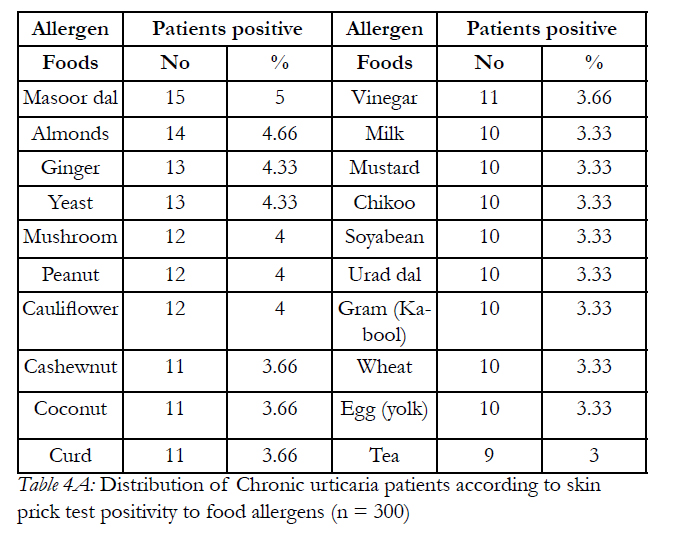
Table 4A: Distribution of Chronic urticaria patients according to skin prick test positivity to food allergens (n = 300).
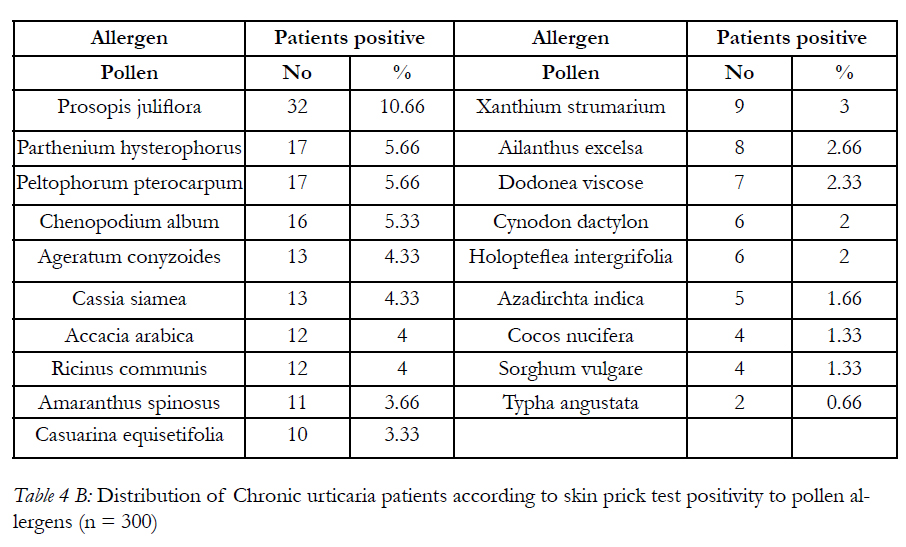
Table 4 B: Distribution of Chronic urticaria patients according to skin prick test positivity to pollen allergens (n = 300).
Among dust mites, 42 (14%) and 39 (13%) were sensitive to Dermatophagoides farinae & Dermatophagoides pteronyssinus respectively.
Among dusts, majority of patients, 17(5.66%) were sensitive to House dust, followed by Paper dust 12(4%), wheat dust 10(3.33%), cotton dust 6(2%) and hay dust 3(1%).
Among fungi, majority of patients i.e., 11(3.66%) were sensitive to Candida albicans, followed by Aspergillus fumigatus 10(3.33%), Cladosporium herbatum 7(2.33%), Penicillium Sp 6(2%) and others (i.e.,Alternaria alternate 5(1.66%), Aspergillus flavus 4(1.33%), Trichoderma 4(1.33%), Curvularia lunata 2(0.66%), Helminthosporum 1(0.33%) and Aspergillus niger 1(0.33%).
Among insects, majority of patients 21(7%) were sensitive to Housefly followed by Cockroach 10(3.33%), Mosquito 10(3.33%) and others. Among epithelia, 6 (2%), 5 (1.66%) & 4 (1.33%) were sensitive to Dog epithelia, Buffalo dander & Sheep’s wool respectively.
Discussion
In the present study, the mean age of chronic urticaria patients was 35.15 ± 12.96 years. This is in accordance with the findings of Priya HA et al [7] where the mean age was 35.7 years.
In the present study, maximum i.e., 60.33% were having chronic urticaria alone. The other co-morbid conditions associated with chronic urticaria were chronic urticaria with conjunctivitis among 14.33% of patients followed by chronic urticaria with allergic rhinitis among 11.33% and chronic urticaria with conjunctivitis & rhinitis among 7%. This observation is in accordance with the findings of Hari Priya et al [7], where 54.9% of patients were having chronic urticaria alone, 22.4% had chronic urticaria and allergic rhinitis and 23% had chronic urticaria with asthma.
Majority of chronic urticaria patients were having symptoms from 6 weeks to one year in the present study, whereas majority of patients were having symptoms of chronic urticaria from 1 to 4 years in the study conducted by Priya HA et al [7].
In the present study, 14.67% of chronic urticaria patients had a family history of atopy, which was lower than the findings of Anuradha et al [15] where 31.8% of chronic urticaria patients had family history of atopy.
In Chronic urticaria patients, Rhinitis and Asthma were other atopic diseases also affected by food allergens. [4] Similar findings was observed in the present study.
In the present study, majority 164 (54.66%) of the chronic urticaria patients (with or without co morbid conditions) were sensitive to food allergens. The most common foods for which they were sensitive were Masoor dal, Almond, Ginger and Yeast. Whereas in the study conducted by Priya HA et al [7], majority were sensitive to beans, mustard, cardamom, cashew and ginger. In the study conducted by Por Alvarado MI [16], the principal foods involved in allergic reactions were fruits (57.7%), tree nuts (23.9%) and crustaceans (12.7%) in adults and fruits (54.2%), tree nuts (20%), legumes (14.3%) and fish (14.3%) in children.
Majority of the patients were sensitive to Prosopis juliflora (10.66%), followed by Parthenium hysterophorus (5.66%), Peltophorum pterocarpum (5.66%) and Chenopodium album (5.33%). It differs from the study conducted by Anuradha et al [15], where the predominant pollen allergens in urticaria were Sorghum vulgare (64.7%) followed by Pennisetum typhoides (56.7%) and Artemesia scoparia (51.9%). Though the studies [6-9] implicated house dust mites and foods sensitivity in chronic urticaria based on skin prick testing and in vitro analysis, in the present study, in addition to house dust mite and food sensitivity, majority of patients have also shown sensitivity to pollens.
In the present study, 14% & 13% of patients were sensitive to Dermatophagoides farinae & Dermatophagoides pteronyssinus respectively. This is in accordance with the other studies [6,8,9,17]. Studies [8, 9] have also shown a significant association between house dust mite sensitivity and chronic urticaria using intradermal and in vitro testing.
The study conducted by Tanaka et al [18] suggested the route of entry of the house dust mite allergens into the skin tissues to interact with specific IgE on mast cells. Numata [9] has also discussed the hypothesis of Hannafin that the dust mite antigen could penetrate the stratum corneum based upon its molecular weight.
To conclude, this study suggests a possible association/ role of pollens sensitivity with chronic urticaria in addition to foods & dust mites sensitivity. It is important to perform skin prick tests among patients suffering from chronic urticaria (with or without comorbidities) not only for food allergens but also for pollens, house dust mites and other allergens for diagnosis and proper management. Since there seem to be geographical differences is the prevalence of allergens causing allergy, there is a need to carry out more such studies in different regions.
References
- Black AK, Champion RH. Urticaria. In: Champion RH, Burton JL, Burns DA, Breathnach SM, editors, Rook/Wilkinson/ Ebling. Textbook of Dermatology. 6th Ed. London: Blackwell Science; 1998.p.2113-39.
- Barlow RJ, Ross EL, Mac Donald DM, Kobza Black A, Greaves MW. Mast cells and T lymphocytes in chronic urticaria. Clin Exp Allergy 1995;25:317-22.
- Sveum RJ. Urticaria. The diagnostic challenge of hives. Postgrad Med 1996 Aug;100(2):77-78, 81-84.
- Jackson WF. Food Allergy. ILSI Europe Concise Monograph Series. International life Sciences Institute; 2003.p.3-35.
- Greaves MW. Chronic urticaria. N Engl J Med 1995;332:1762-72.
- Mahesh PA, Kushalappa PA, Holla AD, Vedanthan PK. House dust mite sensitivity is a factor in chronic urticaria. Indian J Dermatol Venereol Leprol 2005;71:99-102.
- Priya HA, Anuradha B, Vijayalakshmi VV, Latha SG, Murthy KJR. Profile of food allergens in urticaria patients in Hyderabad. Indian J Dermatol 2006;51(2):111-14.
- Sumimoto A, Ishizu K, Takahashi H, Yamada S, Numata T, Yamamoto S, et al. Correlation between Dermatophagoides Pteronyssinus and Dermatophagoides Farinae House dust mites in Chronic urticaria. Hiroshima J Sciences 1981;30:247-50.
- Numata T, Yamamoto S, Yamura T. The role of mite, house dust and candida allergens in chronic urticaria. J Dermatol 1980;7:197- 202.
- Antonicelli L, Micucci C, Voltolini S, Feliziani V, Senna GE, Di Blasi P et al. Allergic rhinitis and asthma comorbidity: ARIA classification of rhinitis does not correlate with the prevalence of asthma. Clin Exp Allergy 2007 Jun;37(6):954-60.
- Bousquet J, Clark TJ, Hurd S, Khaltaey N, Lenfant C, O’bryne P et al. GINA guidelines on asthma and beyond. Allergy 2007 Feb;62(2):102-12. 1
- Tripathi DM. Role of allergen testing and immunotherapy in the management of respiratory allergic diseases. Bombay Hospital Journal.2002; 44(3): 419-25.
- Tripathi DM. Status of skin testing and specific immunotherapy in management of Asthma. Bombay Hospital Journal 1994; 36(1):164-71
- Agarwal MK, Gupta S, bansal SK, Vijayan VK. Cross reacting and unique allergenic components in insect extracts used for the diagnosis and immunotherapy of patients suffering with respiratory allergy. In: Sarma PU, Singh BP, Rao DN et al eds. Trends in Clin Biochem and Lab. Med., Association of Clinical Biochemists, Delhi, India, 2003; 314-24.
- Anuradha B, Vijayalakshmi VV, Latha SG, Priya HA, Murthy KJR. Profile of pollen allergies in patients with asthma, allergic rhinitis and urticaria in Hyderabad. Indian J Chest Dis Allied Sci 2006;48:221-22.
- Por Alvarado MI, Perez M. Study of food allergy on Spanish population. Allergol immunopathol (Madr) 2006;34:185-93.
- Dixit IP. Dust mite urticaria. Practitioner 1973:210:664.
- Tanaka Y, Anan S, Yoshida H. Immunohistochemical studies in mite antigen induced patch test sites in atopic dermatitis. J Dermatol Sci 1990;1:361-8.





