Floating Dislocated Elbow: A Case Report
El Ayoubi A*, Maanouk R, Krite A, El Ghadraoui R, Lahsika M, Benssassi A, Senhaji S, El Idrissi M, El Ibrahimi A, Elmrini A
Department of Osteoarticular Surgery B4, HASSAN II Teaching Hospital, Fez, Morocco.
*Corresponding Author
El Ayoubi A,
Department of Osteoarticular Surgery B4,
HASSAN II Teaching Hospital, Fez, Morocco.
E-mail: abdelghanielayoubi122@gmail.com
Received: April 28, 2017; Accepted: May 09, 2017; Published: May 23, 2017
Citation: El Ayoubi A, Maanouk R, Krite A, El Ghadraoui R, Lahsika M, et al., (2017) Floating Dislocated Elbow: A Case Report. Int J Bone Rheumatol Res. 4(1), 65-67. doi: dx.doi.org/10.19070/2470-4520-1700014
Copyright: El Ayoubi A© 2017. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Floating dislocated elbow is an extremely rare injury, only a few cases were reported. We present here a case of the constellation of skeletal trauma which associates a proximal humerus fracture, distal radius fracture and elbow dislocation. Through the literature review we will include clinical, radiological, therapeutic and functional results of this injury.
2.Case Report
3.Discussion
4.Conclusion
5.References
Introduction
Stanitski and Micheli introduced for the first time in 1980 the floating elbow as an ipsilateral supracondylar humerus and forearm axis fractures that disconnect the elbow from the remaining limb in children [1]. This description has been extended to adults who define concomitant fractures of the humerus and forearm in the same extremity [2], but the more uncommon is floating dislocated elbow [3, 4]. Only a few cases of this injury were reported in the literature [5-7]. We set forth a case of a floating dislocated elbow, the clinical, radiological aspects and the management problems of this injury.
Case Report
A 24-years-old man was attended at the emergency room after a work accident; he fell to the ground from a height of 4m and landed on his left side. At the physical examination, the left arm and forearm were swollen, deformed, and he was in pain, with no neurovascular and no cutaneous damage (Figure1). The patient x-rayed the upper limb which showed a surgical cervical fracture of the humerus and a fracture of the distal extremity of the radius with a postero-external elbow dislocation (Figure 2).
After associated injuries of head, spine, and abdomen had been excluded, in the first instance the patient had a reduction of elbow dislocation. In the second instance the patient had humeral plating, and fixation of the distal radial fracture using the Kapandji intrafocal K-wire technique (Figure 3).
The arm was immobilized using a well-padded above-elbow plaster in 90° elbow flexion for three weeks. The patient was then encouraged to begin the rehabilitation of the elbow, shoulder and wrist: a complete flexion and extension of elbow was allowed, at that time, the patient was allowed to perform muscle strengthening exercises of the upper limb and joint range of motion.
Bone union was demonstrated radiographically 2 months postoperatively. At the 6th month, the elbow showed full range of motion in flexion and extension, as well as in pronosupination. The muscular trophism was similar to that of the contralateral upper arm. The patient didn't complain of pain. The functional outcome assessed using the Constant shoulder score [8] and the Mayo elbow performance score [9] was excellent.
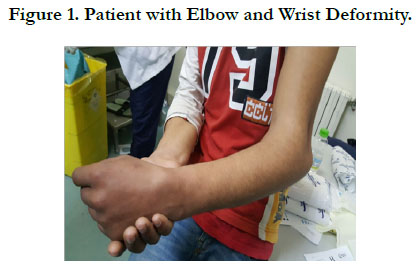

Figure 1. Patient with Elbow and Wrist Deformity.
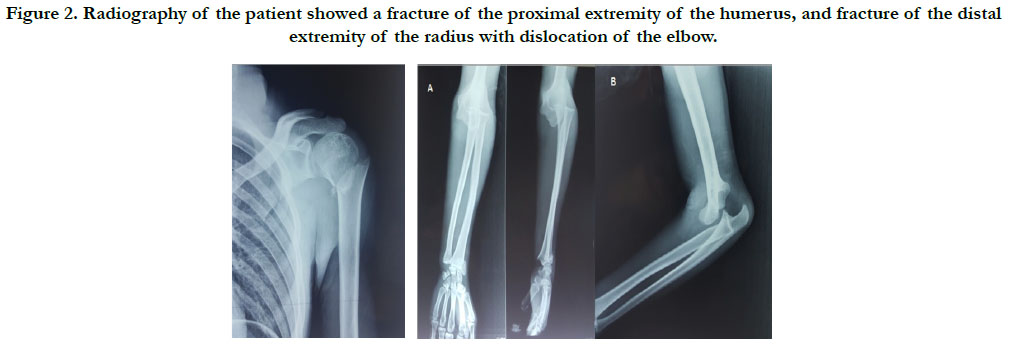
Figure 2. Radiography of the patient showed a fracture of the proximal extremity of the humerus, and fracture of the distal extremity of the radius with dislocation of the elbow.

Figure 3. Radiological Control after Reduction and Osteosynthesis of the Different Injuries.
Discussion
Floating dislocated elbow is an uncommon injury, even if it's an isolated lesion. These injuries are generally a consequence of a high energy trauma; the outcomes are variable and related to both the severity of the initial trauma and the treatment applied [10].
The present case involves the association of humerus proximal fracture and posterolateral dislocation elbow and radius distal fracture which made the whole upper limb unstable. It was extremely difficult to determine the exact mechanism of trauma from the patient history.
The classic mechanism of dislocation elbow is a fall on an outstretched arm, and of a typical posterolateral elbow dislocation is an elbow that has been loaded axially in a valgus position with the forearm supinated [11]. In this case, the patient fell from a height of 4m, the remaining forces caused the radius distal fracture and humeral proximal fractures.
Several treatment modalities have been reported for the floating dislocated elbow, mainly related to the humerus, including: closed reduction and cast, open reduction and internal fixation, intramedullary nailing, and external fixation [2, 10, 12, 13].
Rogers et al., [10] reported 100% nonunion rate in humerus fractures without rigid fixation. Yokoyama et al., [2] recommended stable internal fixation after reviewing 14 cases. Simpson and Jupiter [14] stated in their review article that when the floating elbow affects the joint, open reduction and internal fixation is advisable. De Carli et al., [15] based on their case report and review of the literature made an effort to categorize ‘‘floating dislocated elbow’’ injuries according to severity and morphologic complexity:
Type I: Floating dislocated elbow without articular bone injury [4-10].
Type II: Floating dislocated elbow with distal radioulnar joint dislocation [3].
Type III: Floating dislocated elbow with articular fracture of the distal aspect of the humerus [15].
We have presented a variant of floating dislocated elbow with radius distal fracture, and proximal humeral fracture which is not included in this classification.
Traitement of the case reported includes at the beginning a reduction of elbow dislocation in emergency room, and then a reduction and internal fixation of the proximal humeral fracture and K-wiring of the radius distal fracture. The arm was immobilized using a well-padded above-elbow plaster in 90° elbow flexion for three weeks, and reeducation was begun as soon as the plaster was removed.
Conclusion
Floating dislocated elbow faces up to the orthopedic surgeon to an extremely rare and severe injury with unpredictable outcome, despite adhering to the rule of stable and rigid internal fixation. Adequate initial management of the various lesions allows excellent functional results.
References
- Stanitski CL, Micheli LJ (1980) Simultaneous ipsilateral fractures of the arm and forearm in children. Clin Orthop Relat Res. 153: 218–22.
- Yokoyama K, Itoman M, Kobayashi A, Shindo M, Futami T (1998) Functional outcomes of ‘‘floating elbow’’ injuries in adult patients. J Orthop Trauma. 12(4): 284-90.
- Sarup S, Bryant P (1997) Ipsilateral humeral shaft and Galeazzi fractures with posterolateral dislocation of the elbow: a variant of the ‘‘floating dislocated elbow’’. J Trauma. 43(2): 349–52.
- Viegas SF, Gogan W, Riley S (1989) Floating dislocated elbow: a case report and review of the literature. J Trauma. 29(6): 886–8.
- Levin LS, Goldner RD, Urbaniak JR, Nunley A, Hardaker WT (1990) Management of severe musculoskeletal injuries of the upper extremity. J Orthop Trauma. 4(4): 432-40.
- Fracture and dislocation compendium. - Orthopedic Trauma Association Committee for Coding and Classification. J Orthop Trauma. 10(1): 1-30.
- Papavasiliou V, Nenopoulos S (1986) Ipsilateral injuries of the elbow and forearm in children. J Pediatr Orthop 6(1): 58-60.
- Constant CR, Murley AH (1987) A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res. 214: 160–4.
- Morrey BF (1993) The elbow and its disorders. (2nd edn), Philadelphia: W.B. Saunders Co. 86–97.
- Rogers JF, Bennett JB, Tullos HS (1984) Management of concomitant ipsilateral fractures of the humerus and forearm. J Bone Jt Surg Am. 66(4): 552–556.
- O’Driscoll SW, Morrey BF, Korinek S (1992) Elbow subluxation and dislocation. A spectrum of instability. Clin Orthop Relat Res. 1992(280): 186–97.
- Capomassi M, Slullitel M (2001) Codo flotante del adulto. Rev Asoc Arg Ortop y Traumatol. 66: 99 –105.
- Solomon HB, Zadnik M, Eglseder A (2003) A review of outcomes in 18 patients with floating elbow. J Orthop Trauma. 17(8): 563–570.
- Simpson NS, Jupiter JB (1995) Complex fracture patterns of the upper extremity. Clin Orthop. 318: 43–53.
- De Carli P, Boretto JG, Bourgeois WO, Gallucci GL (2006) Floating dislocated elbow: a variant with articular fracture of the humerus. J Trauma. 60(2): 421-2. http://dx.doi.org/10.1097/01.ta.0000203569. 57055.90.





