Reliability and Validity of an Arabic Version of Quality of life - Alzheimer Disease in Alexandria, Egypt
Shata ZN1*, El-Kady HM2, Ibrahim HK3
1 Lecturer of Mental Health, High Institute of Public Health (HIPH), Alexandria University, Egypt.
2 Assistant Professor of Geriatric Health, High Institute of Public Health (HIPH), Alexandria University, Egypt.
3 Assistant Professor of Public Health Nursing, High Institute of Public Health (HIPH), Alexandria University, Egypt.
*Corresponding Author
Zeinab Nazeeh Shata,
Lecturer of Mental Health, Family health Department,
High Institute of Public Health (HIPH),
Alexandria University, Egypt.
Tel: +2 01007978715
E-mail: zeinab.shata@yahoo.com
Article Type : Research Article
Received: August 20, 2015; Accepted: October 15, 2015; Published: October 19, 2015
Citation: Shata ZN, El-Kady HM, Ibrahim HK (2015) Reliability and Validity of an Arabic Version of Quality of life - Alzheimer Disease in Alexandria, Egypt. Int J Behav Res Psychol, 3(8), 156-162. doi: dx.doi.org/10.19070/2332-3000-1500028
Copyright: Shata ZN© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objectives: Quality of life has been currently recognized as a highly important outcome measure in the management of dementia. This work aimed to examine the psychometric properties of an Arabic-translation of Quality of life-Alzheimer
Disease scale (QoL-AD) for patient and caregiver reports in Alexandria, Egypt.
Methods: A total of 100 patient-caregiver dyads who attended the psycho-geriatric out-patient clinic of El-Mammora Mental Hospital in Alexandria participated in a cross sectional study. Tools included the Mini Mental State Examination (MMSE), Katz Index for Activities of Daily Living (ADL), the Patient Health Questionnaire-9 (PHQ-9), and the QoL-AD.
Results: Both patients and caregivers reports showed satisfactory internal consistency (Cronbach’s alpha coefficient > 0.70). The correlation between patient and caregiver ratings was very good (Rho= 0.75, p≤ 0.001). All validity measures used (PHQ-9, ADL) revealed good convergent validity of the Arabic version. The principal component factor analysis supported the construct validity of the scale.
Conclusion: The Arabic version of QoL-AD is a reliable and valid tool in people with dementia with a MMSE of 10 or
higher.
2.Introduction
3.Methods
3.1.Data Collection tools and techniques
3.2.Statistical Analysis
3.3.Ethical Considerations
4.Results
4.1.Characteristics of participants
4.2.Reliability of the QoL-AD Arabic version
4.3.Validity of the QoL-AD Arabic version
5.Discussion
6.Conclusion
7.References
Keywords
QoL-AD; Dementia; Quality of Life; Alzheimer Disease; Reliability and Validity.
Introduction
Dementia is currently recognized as a major public health challenge in both developed and developing countries attributed to the increased ageing of populations [1].
In a meta-analysis study [2] to estimate the prevalence of dementia from 1980 to 2009, worldwide rates were 5%-7% for those aged ≥ 60 years. In 2010, the number of people with dementia was estimated to be 35.6 million worldwide, and this number is expected to almost double every 20 years. Meanwhile, 58% of all people with dementia lived in low or middle income countries, and this percentage is expected to increase to 63% in 2030 and 71% in 2050 [2].
In Egypt, community based surveys on dementia reported prevalence rates that ranged from 1.4% to 21.95%. Dementia rates in Egypt increases markedly with the older ages [3-5]. The mean age-adjusted prevalence estimate in Egypt is 4.5% [1].
Health related quality of life is considered the main goal for health promotion among elderly in general [6]. The increasing number of elderly means that quality of life (QoL) among people with dementia in the coming years will attract more attention. With no cure to dementia, the main concern becomes how to maximize QoL in people living with dementia [7, 8]. Moreover, several studies considered QoL as a highly important outcome measure in the management of dementia [7, 9, 10].
Review of literature indicated that all reports on the QoL in people with dementia came from the work of Lawton in 1991 [8]. Lawton [11] stressed the multidimensionality of the QoL and the need to assess it subjectively as well as objectively. Several instruments based on Lawton's model of QoL were designed to measure QoL in dementia patients. They varied in content, type of respondent, administration method, and targeted population [12]. There is a continuing debate on the validity and meaningfulness of the self-report of quality of life by people with dementia due to concerns about memory and other cognitive impairments influence on the ‘accuracy’ of reporting [13-15]. Logsdon et al, [16] included patient and proxy appraisal in their Quality of life- Alzheimer Disease (QoL-AD) scale which assesses several QoL domains: physical condition, mood, interpersonal relationships, ability to participate in activities, and financial condition.
To the best of our knowledge, the psychometric properties of an Arabic version of QoL-AD have not yet been assessed in Arab countries including Egypt. Thus, the current work aims to examine the reliability and validity of an Arabic-translation of QoLAD for patient and caregiver reports in Alexandria, Egypt.
Methods
A cross sectional study was conducted in the psycho-geriatric out-patient clinic of El-Mammora Mental Hospital in Alexandria; a hospital that is affiliated to the General Secretariat of Mental Health in Egypt. It provides the tertiary level of mental health services for people living in Alexandria Governorate and three other governorates.
The study targeted dementia patients attending the psycho-geriatric clinic and their main caregivers during the period of the study (6 month period during 2013). The clinic was visited during its working days (two days per week) to recruit the minimum required sample size. A minimum of 90 patient-caregiver dyads were required based on QoL-AD mean scores and standard deviations of both elders (31.58 ± 5.88) and their caregivers (27.08 ± 5.85) [17], with a confidence level and a power of 95% for each, and equal patients/caregivers sample size ratio. Total participants were 100 patient-caregiver dyads.
Inclusion criteria included elders diagnosed with dementia by the hospital psychiatrist; living in the community; both patient and caregiver being able to complete the QoL-AD (patients with MMSE less than 10 were excluded), and having one main caregiver accompanying the patient at the time of interview. Only patients whose main caregivers were family members were included in the study for better reporting and for homogeneity of the sample (2 paid caregivers were excluded).
Data were collected from both patients and caregivers through an interview by a one trained psychologist. Basic data included demographic and socio-economic variables. The following tools were used:
It is a clinician administered test used to assess different domains of cognitive functions with a total score of 30. It tests the individual’s registration of new information, orientation, attention and calculation, recall, language, and construction skills.
ADL is used to assess functional status as a measurement of the elderly ability to perform activities of daily living independently. The Index ranks adequacy of performance in the six functions of "bathing, dressing, toileting, transferring, continence, and feeding". Each item receives either "Yes" or "No" for independence on each of the six functions. Scoring is one for each "Yes" and zero for each "No" response.
PHQ is a self-report version of the PRIME-MD diagnostic instrument for common mental disorders [21]. The PHQ-9 is the depression module, which is based on the nine DSM-IV criteria of depression [22]. The nine items are rated on a Likertscale from 0 to 3. It is commonly used to measure depression and its severity in medical populations in clinical settings including people with cognitive impairment and older adults [23]. PHQ-9 assesses depressive symptoms in the last two weeks by self-reporting or patient interview. An Arabic version was validated in an Egyptian study and showed acceptability and good psychometric properties [20].
It is a brief measure of quality of life among people with dementia that can be completed by either patient or caregiver or both. Areas assessed in the scale include: physical health, energy, mood, living situation, memory, family, marriage, friends, self as a whole, ability to do chores around the house, ability to do things for fun, money, and life quality as a whole. The scale consists of 13 items, each is rated on a four point scale, with 1 being poor and 4 being excellent. Total scoring is obtained by summing all items and it ranges from 13 to 52. Evaluation is based on patient's or caregiver's reports or both. The combined report is calculated by multiplying patient's scores by 2, then adding caregiver's scores and finally dividing the sum of both by three. This composite score gives more weight to patients' reports than the caregivers' since patients are the main target for evaluation by the scale. This scale is best applied to patients with MMSE 10 or higher.
An Arabic-translated version of this questionnaire was developed, checked and confirmed through forward/backward translation. The acceptability and wording of the Arabic version were tested in a pilot sample of 10 patients and caregivers. The final Arabic version was then introduced to the study participants for further validation.
The Kolmogorov-Smirnov goodness-of-fit test was used to test normality of the distribution.
Reliability of the scale was measured by testing item-total correlation as well as the correlation between scale items and the general item-13 "Life as a whole" for both patient and caregiver reports separately. Cronbach alpha coefficient was used to test the internal consistency of patient and caregiver reports. Alpha coefficient value from 0.7 to 0.9 is considered satisfactory. Agreement between patient-and caregiver-rated QoL was examined by testing the correlation between patient and caregiver- reports for items and total score.
Validity measures included convergent validity and factor analysis. Convergent validity was based on the correlation between the patient, and caregiver reports with other three validity measures that should be theoritically correlated with; including PHQ-9 for depression, ADL for functional independence, and QoL-AD (combined report-total).
Principal component factor analysis with varimax rotation was conducted for both patient and caregiver reports. KMO and Bartlett's test of sphericity were used to test for the appropriatenessof factor analysis. Significant Bartlett’s test of sphericity and KMO values greater than 0.5 indicated appropriateness. The eigenvalue was greater than 1 [24].
All correlations were carried out using Spearman's Rho. For all statistical analyses, P-values of 0.05 or less were considered significant.
The Statistical Package for Social Sciences (SPSS, version 16; SPSS Inc., Chicago, USA) was used for data analysis.
The study was approved by the Ethics Committee at the High Institute of Public Health (HIPH) – Alexandria University on the basis of the Declaration of the Helsinki and from the General Secretary of Mental Health Ethical Committee. Objectives of the study were explained to participants and verbal consents were obtained from them thereafter.
Table 1 shows socio-demographic characteristics of the sample. The age of dementia patients ranged from 51 to 84 years with a mean of 67.61 ± 6.41 years. Females outnumbered males (56%), 32% were married and 67% were widowed, single, or divorced. Nearly 70% were illiterates or could just read and write, while 6% were university graduates. The majority of patients (92%) considered their income as adequate.
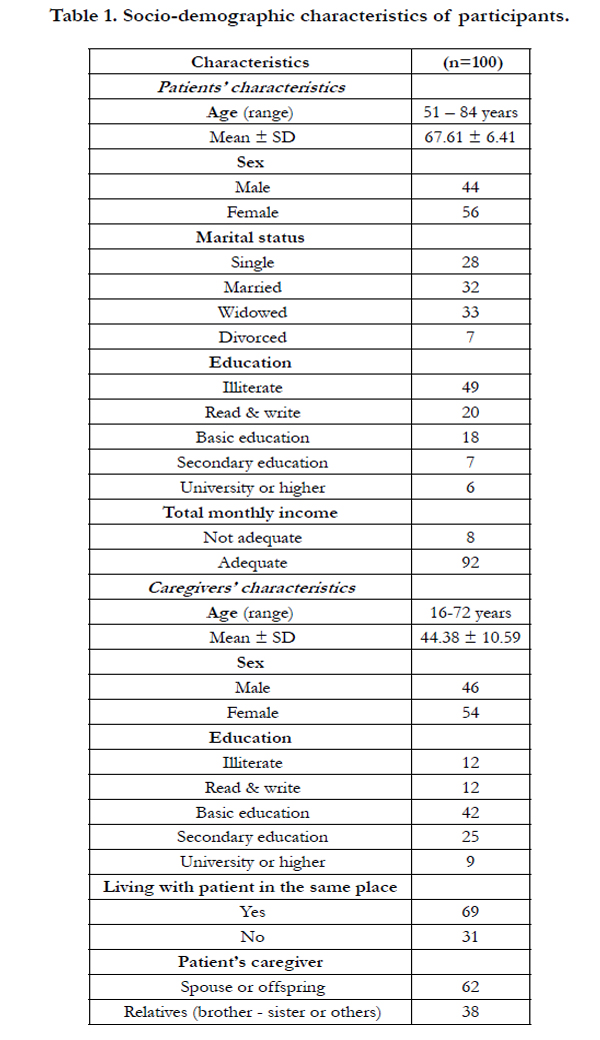

Table 1. Socio-demographic characteristics of participants.
Concerning caregivers' characteristics, their age ranged from 16 to 72 years with a mean of 44.38 ± 10.59 years. Nearly half of them (54%) were females and more than two thirds (69%) lived with the patient in the same place. In contrast to patients' educational level, 76% of caregivers completed their basic education or higher. Nearly two thirds (62%) of caregivers were spouses or offspring.
Patients' scores on the MMSE ranged from 10 to 18 with a total mean score of 11.86 ± 1.97. Total mean scores of both patients', caregivers' and combined reports of QoL-AD were 26.67± 3.06, 25.83 ± 3.31, and 26.63 ± 2.65, respectively.
As shown in Table 2, item-total correlations ranged from 0.20 to 0.65 for patients, 0.22 to 0.86 for caregivers. All correlations were statistically significant (p ≤ 0.05). When items correlated with item-13, all of them showed significant correlations except for "living situation" and "ability to do things for fun" in both patient and caregiver reports. Additional three items in the caregiver report did not show statistically significant correlation with item- 13; "energy", "marriage", and "ability to do chores around the house". The patient and caregiver reports of the Arabic version showed good internal consistency (Cronbach’s alpha coefficient = 0.77, and 0.84, respectively).
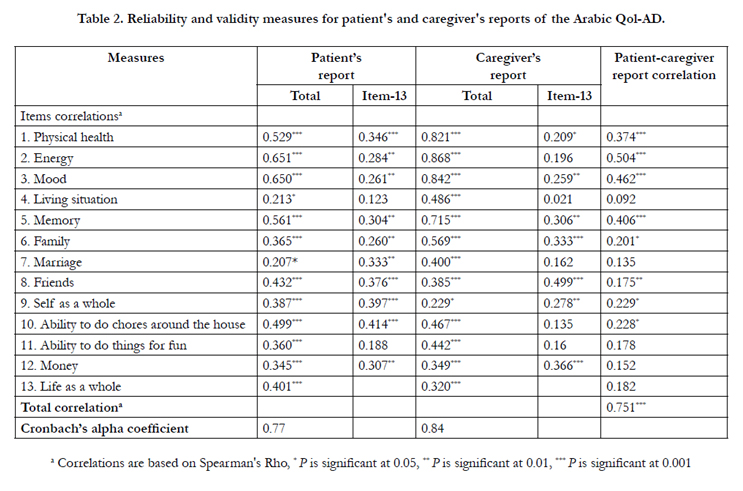
Table 2. Reliability and validity measures for patient's and caregiver's reports of the Arabic Qol-AD.
The agreement between patient and caregiver reports as tested by patient-caregiver report correlation revealed significant positive total correlation (Rho= 0.751, p ≤ 0.001). Five items of the scale did not correlate significantly between patient and caregiver reports, namely; "living situation", "marriage", "ability to do things for fun", "money", and "life as a whole". The statistically significant correlation between items ranged from 0.17 to 0.50 (p ≤ 0.05).
Convergent validity of the scale was assessed by testing the correlation between the patient and caregiver report with PHQ-9 for depression, ADL for functional independence, and QoL-AD (combined report-total) (Table 3).
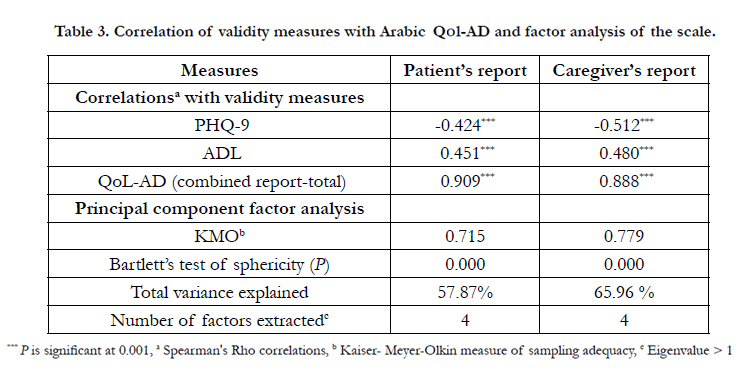
Table 3. Correlation of validity measures with Arabic Qol-AD and factor analysis of the scale.
PHQ-9 showed moderate negative correlation with patient, and caregiver report (Rho= -0.42, -0.51, respectively, p ≤ 0.001), while ADL correlated positively with same reports (Rho= 0.45, 0.48, respectively, p ≤ 0.001). The combined report of QoL-AD showed strong significant correlation with both patient and caregiver reports (Rho= 0.90, 0.88 respectively, p ≤ 0.001). All validity measures used, revealed good convergent validity of QoL-AD Arabic version.
Table 2 shows also the principal component factor analysis of QoL-AD for patient and caregiver. The appropriateness of factor analysis was confirmed by KMO and Bartlett's test of sphericity. Patient's report explained 57.87% of the variance and cargiver report explained 65.96% of it. For both patient and caregiver, four factors were extracted when eigenvalue was greater than 1.
The four extracted factors were rotated by varimax method and correlated with QoL-AD scale items. Loading of the items on rotated factors and variance explained by each factor are presented in Table 4.
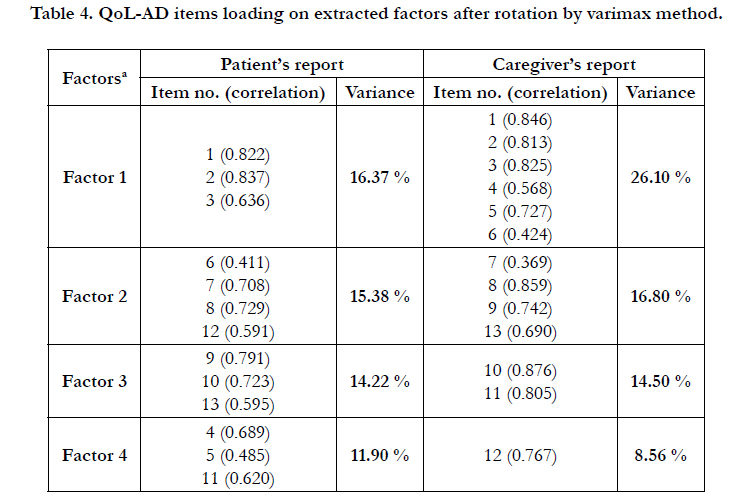
Table 4. QoL-AD items loading on extracted factors after rotation by varimax method.
For the patient's report, factor 1 was loaded by three items that best describe "physical and psychological health". Factor 2 included three items that reflect "interpersonal relationships" and one item for "financial situation". Items loaded on factor 3 can be categorized as "overall assessment of self and life", and "participation in daily activities". The remaining three items loaded on factor 4 reflect three different themes; "surrounding environment", "health", and "participation in daily activities". All items reflecting the same theme were grouped together in patient's report, except for three items. The "memory" item that loaded on factor 4 and it fits best to factor 1 under theme of "physical and psychological health"; and the two items reflecting participation in daily activities where they loaded on two different factors; 3 and 4.
Regarding caregiver's report, six items loaded on factor 1 and they represent "physical and psychological health" by four items, "surrounding environment" by one item, and one item for "interpersonal relationships". The four items grouped in factor 2 describe two themes; "interpersonal relationships" and "overall assessment of self and life". Factor 3 represents the theme of "participation in daily activities", while factor 4 shows the "financial situation". For the caregiver's report, all items related to the same theme were grouped together except the item of "family" which loaded on factor 1 and it should be grouped with the other two items of "interpersonal relationships" on factor 2.
Although themes of factors differed between patient and caregiv er, however items related to each other were grouped together in both reports.
Discussion
It was recognized that in addition to specific symptom treatment of dementia, the main question in care becomes how to promote well-being and maintain an optimal QoL for people with dementia [8, 25].
It is important to find a tool to assess QoL that is brief, easily administered and the most important can incorporate both patient and caregiver ratings either separately or combined. All these criteria apply to QoL-AD, which make it a very suitable tool to be applied in monitoring QoL for people with dementia attending the out-patient clinic.
This work adds to the several versions of QoL-AD that have been validated in different languages worldwide [26-29], by examining the psychometric properties of an Arabic version of QoL-AD. Reliability and validity of the Arabic version have been established in this study.
Although the majority of patients were poorly educated, they could rate their QoL reliably through interview, which indicates the good understandability of the questions. This finding was also supported by Yu et al [30] in their validation of the Chinese version of QoL-AD. The current findings also support the application of QoL-AD to patients with MMSE of 10 or higher, a finding that agrees with the original research [16].
The Arabic scale showed cohesive structure as shown by good internal consistency of patients' and caregivers' reports (Cronbach alpha coefficient = 0.77, and 0.84, respectively) and by correlations of items with the total and with item-13. Reliability of the caregiver's ratings was more satisfactory than the patient's selfratings as evidenced by the higher internal consistency and higher item-total correlations.
In addition, high agreement between patients' and caregivers' reports was found, except five items that did not correlate significantly between the two reports. This disagreement shows that these items (living situation, marriage, ability to do things for fun, money, and life as a whole) are reflecting more subjective than objective measures for QoL.
In partial agreement with the original research [16], five items also did not show significant correlation between patients and caregivers, three were similar to current findings (living situation, marriage, and ability to do things for fun), while the other two (memory and ability to do chores around house) showed significant correlation in the current study. In another study to validate the Chinese version of QoL-AD [30], caregivers reported three items (physical health, living situation, and life as a whole) that differed significantly from the patients. Two of these items were consistent with the current findings. Among all items, "living situation" showed consistent disagreement among the three studies which draws attention to revise or modify this item.
Many studies [7, 31-33] documented the association between depression and QoL among people with dementia and it was suggested as the most common predictor of quality of life in dementia as rated by patients or caregivers, among all settings, and for different types of QoL measures. In addition, the correlation between activities of daily living (ADL) and QoL among people with dementia and specifically with QoL-AD scores has been documented in several studies [16, 25, 33].
These two constructs correlated significantly and as expected with the patient and caregiver reports of QoL-AD, which therefore supports the construct validity of the Arabic version. Another evidence for convergent validity comes from the significant positive correlation between the patients' or caregivers' reports and the combined report of the QoL-AD Arabic version. The caregiver ratings showed higher correlations with depression and ADL than patients, while patients' reports correlated higher with the combined report than did caregivers' ratings. This is expected since the combined report gives more weight to patients' ratings than caregivers'.
The construct validity of the Arabic scale was further supported by findings from the factor analysis of patients' and caregivers' reports. Four factors were obtained for both patients and caregivers that explained 57.87% and 65.96% of variance, respectively. Items loading on rotated factors revealed six different themes for both patients and caregivers. These themes are "physical and psychological health", "interpersonal relationships", "financial situation", "overall assessment of self and life", "participation in daily activities", and "surrounding environment". These themes are in consistency with those mentioned by Logsdon et al. (1999) in their original research [16].
Current findings are partially consistent with those found by Gómez-Gallego et al [29] in their validation of the Spanish version, through factor analysis for patients' ratings only and they obtained 3 factors that explained 61.30% of the total variance. These factors were interpreted as follows: health factor, social relations and environment factor and functional capacity factor.
Although themes represented on each factor differed between patients and caregivers, items belonging to each theme were grouped together in both reports. Moreover, items in the caregivers' reports fitted better on the four factors than in patients' reports, where three items in patients' reports loaded on unrelated factors compared to one item only in the caregivers' reports.
Limitations of the current study include unmatched socio-demographic characteristic between patients and caregivers such as differences in educational level which may be one factor that can affect ratings by both of them. Also this study did not include institutionalized patients or those in advanced stages.
Conclusion
The Arabic version of QoL-AD is proved to be a reliable and valid tool to monitor quality of life among dementia patients attending the out-patient clinic. Patients scoring at least 10 on the MMSE can rate their QoL reliably. The caregivers' reports showed better reliability and validity than patients' reports. So, it is recommended to use the combined scores whenever possible in order not to miss patients' self-ratings. If not applicable, caregivers' reports are more recommended for rating the QoL among people with dementia using QoL-AD. Further research is strongly needed to examine factors that may associate with differences in ratings between patients and caregivers. In addition, the psychometric properties of this scale should be confirmed for use among institutionalized patients and those in advanced stages.
References
- Benamer HT (2014) Neurological disorders in the Arab world. Switzerland: Springer International Publishing.
- Prince M, Bryce R, Albanese E, Wimo A, Ribeiro W, et al. (2013) The global prevalence of dementia: a systematic review and metaanalysis. Alzheimers Dement 9(1):63-75.e2.
- Farrag A, Farwiz HM, Khedr EH, Mahfouz RM, Omran SM (1998) Prevalence of Alzheimer's disease and other dementing disorders: Assiut-Upper Egypt study. Dement Geriatr Cogn Disord 9(6):323-328.
- El Tallawy HN, Farghaly WM, Metwaly NA, Rageh TA, Shehata GA, et al. (2010) Door-to-door survey of major neurological disorders in Al Kharga District, New Valley, Egypt: methodological aspects. Neuroepidemiology 35(3):185-190.
- Tallawy HN, Farghaly WM, Rageh TA, Shehata GA, Badry R, et al. (2013) Door-to-door survey of major neurological disorders (project) in Al Quseir City, Red Sea Governorate, Egypt. Neuropsychiatr Dis Treat. 9:767-771.
- Centers for Disease Control and Prevention. Health-related quality of life (HRQOL) concepts. Centers for Disease Control and Prevention. www.cdc.gov/hrqol/concept.htm.
- Beerens HC, Zwakhalen SM, Verbeek H, Ruwaard D, Hamers JP (2013) Factors associated with quality of life of people with dementia in long-term care facilities: a systematic review. Int J Nurs Stud 50(9):1259-1270.
- Ettema TP, Dröes RM, de Lange J, Ooms ME, Mellenbergh GJ, et al. (2005) The concept of quality of life in dementia in the different stages of the disease. Int Psychogeriatr 17(03): 353- 370.
- Moniz-Cook E, Vernooij-Dassen M, Woods R, Verhey F, Chattat R, et al. (2008) A European consensus on outcome measures for psychosocial intervention research in dementia care. Aging Ment Health 12(1):14-29.
- Rabins PV, Black BS (2007) Measuring quality of life in dementia: purposes, goals, challenges and progress. Int psychogeriatr 19(03):401-407.
- Lawton M. P (1991) A multidimensional view of quality of life in frail elders. The concept and measurement of quality of life in the frail elderly 4-27.
- Ready RE, Ott BR (2003) Quality of life measures for dementia. Health Qual Life Outcomes 1(11):1-9.
- Smyth KA, Neundorfer MM, Koss E, Geldmacher DS, Ogrocki PK, et al. (2002) Quality of life and deficit identification in dementia. Dementia 1(3):345-358.
- Ready RE, Ott BR, Grace J (2006) Insight and cognitive impairment effects on quality-of-life reports from mild cognitive impairment and Alzheimer's disease patients. Am J Alzheimers Dis Other Demen 21(4):242-248.
- Woods RT, Nelis SM, Martyr A, Verhey F, Chattat R, et al. (2014) What contributes to a good quality of life in early dementia? Awareness and the QoL-AD: a cross-sectional study. Health Qual Life Outcomes 12:94.
- Logsdon RG, Gibbons LE, McCurry SM, Teri L (1999) Quality of life in Alzheimer’s disease: patient and caregiver reports. J Ment Health Aging 5(1):21-32.
- Huang HL, Chang MY, Tang JS, Chiu YC, Weng LC (2009) Determinants of the discrepancy in patient- and caregiver-rated quality of life for persons with dementia. J Clin Nurs 18(22): 3107-3118.
- El-Okl M. A, El Banouby M. H, El Etrebi A (2002) Prevalence of Alzheimer dementia and other causes of dementia in Egyptian elderly. MD thesis, Faculty of Medicine, Ain Shams University.
- Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW (1963) Studies of illness in the aged. The index of ADL: A standardized measure of biological and psychosocial function. JAMA 185:914-919.
- Kandil HM (2005) Study of risk factors predicting the co-morbidity between bipolar disorder and anxiety disorders in a sample of Egyptian patients [dissertation]. Alexandria: University of Alexandria.
- Spitzer RL, Kroenke K, Williams JB, Patient Health Questionnaire Primary Care Study Group (1999) Validation and utility of a self-report version of PRIME-MD: the PHQ (Patient Health Questionnaire) primary care study.JAMA 282(18):1737-1744.
- Kroenke K, Spitzer RL, Williams JB (2001) The PHQ-9: validity of a brief depression severity measure. J Gen Int Med 16:606-613.
- Hancock P, Larner AJ (2009) Clinical utility of Patient Health Questionnaire- 9 (PHQ-9) in memory clinics. Int J Psychiatry Clin Pract 13:188-191.
- Leech, N. L., Barrett, K. C., & Morgan, G. A. (2005). SPSS for intermediate statistics: Use and interpretation. Psychology Press.
- Logsdon RG, Gibbons LE, Mccurry SM, Teri L (2002) Assessing quality of life in older adults with cognitive impairment. Psychosom Med 64(3):510-519.
- Rosas-Carrasco O, Torres-Arreda LP, Guerra-Silla MG, Torres-Castro S, Gutierrez-Robledo LM (2010) Validation of the quality of life in Alzheimer’s disease (QOL-AD) scale in Mexican patients with Alzheimer, vascular and mixed-type dementia. Rev Neurol 51(2):72-80.
- Novelli MMPC, Nitrini R, Caramelli P (2010) Validation of the Brazilian version of the quality of life scale for patients with Alzheimer’s disease and their caregivers (QOL-AD). Aging Ment Health 14(5):624-631.
- Shin HY (2006) A preliminary study on the Korean version of quality of life- Alzheimer’s disease (QOL-AD) scale in community-dwelling elderly with dementia. J Prev Med Public Health 39(3):243-248.
- Gómez-Gallego M, Gómez-Amor J, Gómez-García J (2012) Validation of the Spanish version of the QoL-AD scale in Alzheimer disease patients, their carers, and health professionals. Neurología (English Edition) 27(1):4-10.
- Yu HM, He RL, Ai YM, Liang RF, Zhou LY (2013) Reliability and validity of the quality of life-Alzheimer disease Chinese version. J Geriatr Psychiatry Neurol 26(4):230-236.
- Banerjee S, Samsi K, Petrie CD, Alvir J, Treglia M, et al. (2009) What do we know about quality of life in dementia? A review of the emerging evidence on the predictive and explanatory value of disease specific measures of health related quality of life in people with dementia. Int J Geriatr Psychiatry 24(1):15-24.
- Missotten P, Ylieff M, Di Notte D, Paquay L, De Lepeleire J, et al. (2007) Quality of life in dementia: a 2‐year follow‐up study. Int J Geriatr Psychiatry 22(12):1201-1207.
- Hoe J, Katona C, Orrell, M, Livingston G (2007) Quality of life in dementia: care recipient and caregiver perceptions of quality of life in dementia: the LASER‐AD study. Int J Geriatr Psychiatry 22(10):1031-1036.





