A Case Study Tracking The Cognitive Impact Of Insomnia
Kathy S R1*, Katarzyna L K2
1* Full Professor, Psychology Department, Elmhurst College, Elmhurst, IL USA.
2 Clinical Psychology Student/ The Chicago School, Chicago, IL USA.
*Corresponding Author
Kathy Sexton-Radek,
Full Professor,
Psychology Department, Elmhurst College,
Elmhurst, IL USA & Clinical Psychologist, Behavioral
Health Director, Suburban Pulmonary & Sleep Associates,
Westmont, IL USA.
E-mail: ksrsleep@aol.com
Received: December 18, 2013; Accepted: January 22, 2014; Published: January 24, 2014
Citation: Kathy S R, Katarzyna L K (2014) A Case Study Tracking the Cognitive Impact of Insomnia. Int J Behav Res Psychol. 2(1), 12-14. doi:dx.doi.org/10.19070/2332-3000-140003
Copyright: Kathy S R© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
A case study is used to illustrate cognitive factors related to poor sleep quality in a young adult. The participant was a healthy patient outside of his sleep disturbance. Changes in cognitive functioning were evaluated with the Repeatable Battery for Assessment of Neuropsychological Status (RBANS). The profile of performance for the participant was similar to that previously reported for mild cognitive impairment due to head trauma. The implication to health (i.e., cognitive functioning) for sleep disturbance is presented.
2.Introduction
3.Materials and Methods
4.Results and Discussion
5.References
Keywords
Sleep Deprivation; Cognitive Impairment; Adjustment Disorder of Sleep.
Introduction
Sleep quality in young adults is commonly reported as compromised. Some 10% of young adults meet criteria for a diagnosed sleep condition. With the normal sleep cycle maturing in late teens, choices by many young adults jeopardize the set-up of a regular sleep pattern. Social, academic and vocational schedules are extended by choice with the availability of twenty-four hour contact to resources, people and entertainment. Empirical studies have documented fragmented, insufficient sleep during the school/work week with variable sleep schedules on the weekends (e.g., 4 a.m. bedtime and sleeping until mid-afternoon/napping). The results of these sleep schedules have been found to be reportings of knowledge of their poor sleep, increased minor health problems such as cold and flu. More female than male young adults complain of poor sleep, while both genders, in college performance, equally experience decrements in performance (i.e., lowered GPA). Laboratory studies have documented reduced vigilance, creativity and innovative performance or cognitive testing of young adults reporting poor sleep quality.
Transient insomnia is short term and precipitated by environmental conditions such as stress, travel/time schedule changes, and illness. Difficulty falling asleep or staying asleep (insomnia) is the most commonly reported sleep disturbance. When medical and other sleep disturbance symptoms are ruled out, the etiology of the resultant insomnia are commonly stress factors. For chronic condition of insomnia lasting longer than one month, an underlying psychological condition, common environmental stressors are at the source. In some cases longstanding environmental conditions such as excessive noise or light at night, insufficient light during the day, roommate/pet sleep patterns and poor sleep hygiene perturb sleep quality. In their adjustment to the developmental stage of independence, choices to engage in excessive late night hours, moderate adherence to schedule demands of work/early morning college classes impact the young adult sleeper. The resultant poor sleep quality measured by reductions in sleep schedule make the young adult vulnerable to insomnia sleep disturbance diagnoses.
Cerebral apathy has been demonstrated in animal studies of subjects deprived of sleep. These insomnia simulations resulted in less responsiveness in frontal and parietal regions of the brain [2]. In human participants with natural cases of insomnia, a form of relaxation using sensorimotor rhythm, SMR (12-15 Hz quiet but alert wakefulness), was used during daytime trainings to enhance their sleep. After ten weeks of training, significant differences were measured in the group as compared to controls in terms of the reduced number of awakenings and increased amount of slow wave sleep. The researchers described a SMR training enhancement associated with sleep consolidation. The consolidation of sleep was stated to be associated with overnight memory consolidation and increased sleep spindle changes manifesting a beneficial cognitive effect [3]. Insomnia awakenings often result in cognitive deficits and impairments of nocturnal memory consolidation [4]. Patients with insomnia display hyper- arousal symptoms including fast frequency EEG [4]. Increased metabolism in brain areas during sleep have been measured by PET in insomnia patients [4]; it is believed that this is influential in cognitive deficits in waking and nocturnal memory consolidation. Reductions in hippocampal size have been reported from measurements of insomnia patients [4]. A hyperarousal state is hypothesized to explain insomnia – both its etiology and what sustains the wakefulness. In insomnia, physiological phenomena of increased autonomic activity, activation of neuroendocrine and neuroimmunological axes and increased fast frequencies {4} that both generate and sustain insomnia [4]. In measurements of cognitive functioning in everyday activities such as memory, distractibility blunder and memory for names, insomnia subjects [5]. An increase in insomnia symptoms is associated with an increase in cognitive failures in everyday events [5]. Some researchers have concluded that in addition to cognitive failures, slowed efforts by insomniacs reflects memory decrements secondary to the poor sleep quality [6]. An investigation of insomniac versus healthy controls on memory consolidation tasks, where recovery sleep was made available, identified the insomniacs as having substantially reduced memory consolidation [7]. Brain injury MRI studies reported reduced activation of task-related working memory regions in insomniac patients as compared to age matched controls [8]. The right dorsolateral prefrontal cortex reflected reduced modulation with increasing task difficulty.
In summary, insomnia is a common sleep disturbance characterized by a hyperarousal state of inability to fall or stay asleep. Insomnia is common in the young adult population [1]. Neurobehavioral measures have substantiated the hyper arousability and reduced cognitive functioning behaviors [2, 8]. The current study was designed as a case control study to measure cognitive functioning in a young adult presenting with insomnia. A full description of the patient is provided in Table1.
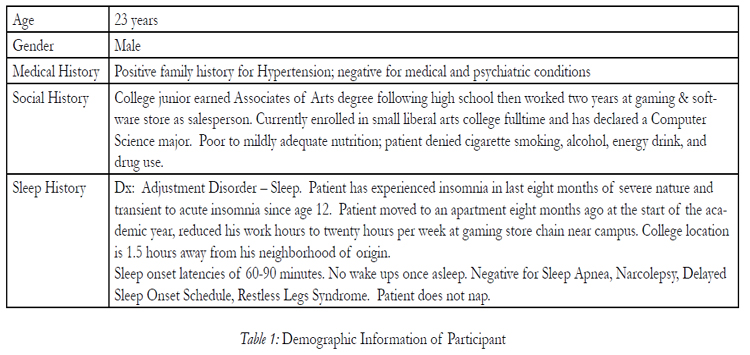

Table 1: Demographic Information of Participant.
Materials and Methods
The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) is a series of 12 subtests that provides a broad selection of tasks that measure neuropsychological impairment. Appendix-I lists further information about the RBANS. Additionally, a standard sleep log was kept that required the daily recording of bedtime, amount to fall asleep, wake up time, time out of bed, nap and naptime.
A patient that presented with insomnia agreed to have his treatment studied and an informed consent was signed. The patient kept a daily sleep log and participated in eight weeks of Cognitive Behavior Therapy (CBT), a collaborative therapy focused on setting an optimal sleep pattern, practicing good sleep hygiene and understanding of the basics of sleep that apply them [1]. (More information on CBT can be found in reference 1.) The RBANS was administered during intake, one month and at six months following the eight weeks of CBT. The total scores for each testing are presented in Table 2.

Table 2: Demographic Information of Participant.
Results and Discussion
The patient’s sleep improved as measured by sleep efficiency. The results are presented in Figure 1. A 85% sleep efficiency is the goal of CBT, thus, the patient’s progress was adequate for the first four weeks, then leveled off. The sustaining of the sleep cycle denotes that the patient was implementing some CBT strategies but not all. It is notable that the patient’s sleep efficiency declined in the last half of the CBT therapy.
The patient’s cognitive functioning is compromised. Reductions in the patient’s scores were greatest across intake to follow-up in areas of List Learning and Story Memory (immediate memory), and List Recognition and Figure Recall (delayed memory). The patient’s cognitive functioning as measured by the RBANS was sustained from intake to follow-up on tasks involving visuospatial/construction (Line Orientation), attention (Coding). The patient’s performance on cognitive tasks of immediate memory and visuospatial / constructional were in the same range as older adults and traumatic brain injury patients. The patient performed better, comparatively, than the norm groups on language and semantic tasks. Of note is the patient’s performance on delayed memory tasks that exceeds the norm groups.


Figure 1: Sleep Efficiency (SE) versus Treatment Session.
In conclusion as aforementioned, a number of young adults have a poor quality of sleep which impacts their cognitive functioning, as can be evidenced in this case study of a young male with sleep difficulties. The patient was asked to keep a sleep log while he underwent 8 sessions of CBT, and his cognitive functioning was assessed with the Repeatable Battery for Assessment of Neuropsychological Status (RBANS) at intake, halfway through the treatment (session 4), and at 6 month follow-up. It is worthwhile to mention that sleep efficiency of the client increased overall from intake to follow-up at 6 months, however it reached the highest peak between session 2 and 3 and then leveled off for the last half of CBT treatment sessions. Therefore, the client’s utilization of the learned CBT techniques appears to result in overall better sleep efficiency as compared to baseline/intake. The results of the patient’s RBANS subtest scores demonstrate that the cognitive abilities most impacted are immediate memory (List Learning and Story Memory) and delayed memory (List Recognition and Figure Recall), as the scores decreased from intake to 6 month follow-up. On the List Recognition subtest (delayed memory), the client’s score was lower at 6 month follow-up than the norms presented for older adults and the tantric brain sample. Similarly on the Story Recall subtest (delayed memory), the patient’s score was lower at 6 month follow-up compared to the tantric brain sample norms. However, the client’s scores on language subtests increased from intake to 6 month follow up and were higher on the Coding subtest, compared to the norms. Thus from the patient’s scores, it is apparent that cognitive abilities such as language skills improved as sleep efficiency increased, whereas other cognitive abilities such as immediate and delayed memory did not show improvement. Hence the implication that sleep disturbance and poor quality of sleep can impact one’s cognitive functioning and is related to overall health and well-being.
References
- K Sexton-Radek (2003). Sleep Quality in Young Adults. New York:The Edwin Melon Press.
- D Dijk (2013). Sensitive to sleep loss or not: Neurons, working memory, insomnia and the heart. Journal of Sleep Research, 22(3), 237- 238.
- M Schabus, DPJ Heib, J Lechinger, H Griessenberg, W Klenesch, APawlizki, A Kung, B Sterman, & K Hoedlmoser (2013). Enhancing sleep quality and memory in insomnia using instrumental sensorimotor rhythm conditioning. Biological Psychology,
- D Riemann, C Kloepfer, & M Berger (2009). Review functional and structural brain alterations in insomnia: Implications for pathophysiology. European Journal of Neuroscience, 29, 1754-1760.
- A Wilkerson, A Boals, & D Taylor (2011) Sharpening our understanding of the consequences of insomnia: The relationship between insomnia and everyday cognitive failures. Cognitive Therapy Research, 36, 134-139.
- RE Schmidt, M Richter, GHH Gendolla, & M Vander Linden (2010). Young poor sleepers mobilize extra effort in an easy memory task: Evidence from cardiovalsular measures. Journal of Sleep Research, 19, 487-495.
- C Nissen, C Kloepfer, B Feije, H Piosczyk, K Spiegelhalder, U Voderholzer, & W Riemann (2011). Sleep-related memory consolidation in primary insomnia. Journal of Sleep Research, 20, 129-136.
- S Drummond (2013). Neural correlates of working memory performance in primary insomnia. Sleep: Journal of Sleep and Sleep Disorders Research, 36(9), 1307-1316.
- K Duff, MR Schoenberg, D Patton, JS Paulsen, JD Bayless, J Meld, JG Scott, & RL Adams (2005). Regression-based formulas for predicting change in RBANS subtests with older adults. Archives of Clinical Neuropsychology, 20, 281-290.
- C McKay, JE Casey, J Wertheimer, & NL Fichtenberg (2007). Reliability and validity of the RBANS in a traumatic brain injury sample. Archives of Clinical Neuropsychology, 22, 91-98.





