To Compare the Efficacy of Phenylephrine and Mephentermine in Maintaining Arterial Pressure During Spinal Anaesthesia in Infra Umbilical Surgeries
Ramesh R1, Balagi D2, Dayananda VP3
1 Assistant Professor, Department of Anaesthesiology, Bangalore Medical College and Research Institute, Bangalore, India.
2 Postgraduate, Department of Anaesthesiology, Bangalore Medical College and Research Institute, Bangalore, India.
3 Associate Professor, Department of Anaesthesiology, Bangalore Medical College and Research Institute, Bangalore, India.
*Corresponding Author
Ramesh R,
Assistant Professor, Department of Anaesthesiology,
Bangalore Medical College and Research Institute, Bangalore, India.
E-mail: balagi20@gmail.com
Received: June 24, 2016; Accepted: August 12, 2016; Published: September 06, 2016
Citation: Ramesh R, Balagi D, Dayananda VP (2016) To Compare the Efficacy of Phenylephrine and Mephentermine in Maintaining Arterial Pressure During Spinal Anaesthesia in Infra Umbilical Surgeries. Int J Anesth Res. 4(9), 331-335.DOI : dx.doi.org/10.19070/2332-2780-1600068
Copyright: Ramesh R© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: It is important to find an effective method to prevent and treat hypotension during subarachnoid block. Hence we compare the bolus doses of Phenylephrine and Mephentermine to treat hypotension post subarachnoid block.
Methods: This randomised study was conducted in 100 patients of ASA I or II physical status undergoing infraumbilical surgeries under subarachnoid block. Patients were randomized into 2 groups of 50 each. Group P-Phenylephrine of 0.1 mg I.V bolus and Group M-Mephenteramine 6mg I.V bolus given when patient develops hypotension >20% basal respectively. Both the groups received 3ml of 0.5% hyperbaric bupivacaine for subarachnoid block. Vital parameters like blood pressure, heart rate and oxygen saturation were recorded. Any side effects observed were also recorded.
Results: The demographic profile were comparable and statistically similar in both the groups. Both the vasopressors were able to maintain blood pressure above the hypotensive values in their respective groups successfully. The number of hypotension episodes was higher in Group P(34%) than Group M(32%) but statistically insignificant. The average number of drug doses required for recovery from hypotension was higher in the Group P(1.41) than Group M(1.25). The number of episodes of bradycardia was higher in the phenylephrine group(16%) than in the mephentermine group(4%).
Conclusion: We conclude that intravenous bolus of phenylephrine and mephentermine are both effectve at maintaining intraoperative blood pressure during spinal anaesthesia in infraumbilical surgeries but mephenteramine is better than phenylephrine in maintaining BP persistently high and has lesser incidence of bradycardia.
2.Methodology
2.1.Statistical Methods
2.2.Significant figures
2.3.Statistical software
3.Results
4.Discussion
5.Conclusion
6.References
Introduction
Subarachnoid block is a major regional technique with a long history of effective use for a variety of surgical procedures. It produces sympathetic block, sensory analgesia and motor block, depending on dose, concentration, or volumes of local anesthetics. Nevertheless, precipitous hypotension and difficulty in controlling the level of analgesia are major disadvantages of spinal block [1].
The most common serious side effects of subarachnoid block are hypotension (33%) and bradycardia (13%) [2, 3]. Systemic vasodilatation induced by sympathetic blockade after spinal anesthesia, resulting in venous pooling of blood and reduction in systemic vascular resistance, has been regarded as the predominant mechanism for hypotension.
The incidence of hypotension has been reported to be as high as 85% in patients undergoing elective caesarean section under spinal anaesthesia [4].
Infact, subarachnoid block has been found to provide faster recovery, superior analgesia and less nausea and vomiting in the immediate postoperative period as compared to general anaesthesia [5].
However hypotension is a frequent intra operative complication that occurs following subarachnoid block and incidence is higher with higher level of block. It is therefore important to find an effective method to prevent and treat hypotension during subarachnoid block.
Patient leg elevation, head down tilt and use of pressure stockings augment venous return and increase cardiac output and may be sufficient to restore blood pressure to an acceptable level [6]. But such methods cannot be practical always. For example within few minutes of subarachnoid block head down tilt cannot be given as the level of block might ascend up.
Thus most of the strategies for decreasing the incidence of hypotension during subarachnoid block have proved far from being satisfactory or reliable. This has shifted the focus to various vasopressor agents for the prevention as well as treatment of subaracnoid block induced hypotension.
Vasopressors used for prophylaxis and treatment of hypotension should fulfil the following criteria i.e., high efficacy, ability to use liberal doses to maintain blood pressure near normal preventing hypotension.
Earlier Ephedrine was considered the sole choice of vasopressor for treatment of spinal hypotension. It has both alpha and beta adrenergic agonistic action, increasing cardiac output, heart rate and systolic blood pressure.
Phenylephrine is the vasopressor which is a short acting alpha agonist and increases blood pressure with a transient reactive bradycardia, responsive to atropine. It can be administered by bolus as well as by infusion, in titrated doses as per the blood pressure response. Mephentermine is an indirect acting vasopressor whose pharmacological action largely results from endogenous release of catecholamines.
The present study is undertaken to treat the hypotension during subarachnoid block in patients under going infra umbilical surgeries, by administration of iv bolus doses of either Phenylephrine or Mephentermine and compare their effects.
Methodology
This randomised study was conducted in 100 patients undergoing infraumbilical surgeries under spinal anaesthesia at Victoria and Vani Vilas Hospital Bangalore. Institutional ethical committee clearance was obtained. Patient consent taken. Patients were randomized into 2 groups of 50 each by using sealed envelope method. Sample size was calculated by keeping the power of the study at 80% and confidence limits at 95%. Group PPhenylephrine of 0.1 mg I.V bolus given when patient develops hypotension >20% of basal BP [8]. Group M– Mephentermine 6mg I.V bolus given when patient develops hypotension >20% basal BP. Both the groups received 3ml of 0.5% hyperbaric Bupivacaine for subarachnoid block.
The inclusion criteria were age group between 18 to 60 years, ASA I or II physical status [7], posted for infraumbilical surgeries. The exclusion criteria were patient refusal for the procedure, level less than T6, patients with significant coagulopathies and other contra-indications for spinal anaesthesia, patients undergoing caeserian section, patients with history of significant systemic disorders (cardiovascular, respiratory or central nervous system).
All patients underwent preanaesthetic evaluation on the previous day of surgery. Basic and necessary investigations were carried out. Patients were premedicated with Tab Ranitidine 150mg and Tab Alprazolam 0.5mg the night before surgery. All patients were fasted for 6 hours. Iv acess obtained with 18G iv cannula and prehydrated with 10ml/kg Ringer Lactate. Drugs and equipment necessary for resuscitation and general anaesthesia were kept ready and standard monitors like Pulse oximetry, ECG, NIBP connected and monitored. Patients positioned in left lateral position for SAB. SAB was instituted in L3- L4 or L2-L3 interspace. Vital parameters like blood pressure (systolic, diastolic and mean), heart rate and oxygen saturation were recorded preoperatively as well as intra-operatively. Any side effects observed were also recorded.
Descriptive and inferential statistical analysis has been carried out in the present study. Results on continuous measurements are presented on Mean ± SD (Min-Max) and results on categorical measurements are presented in Number (%). Significance is assessed at 5 % level of significance. The following assumptions on data is made, Assumptions: 1. Dependent variables should be normally distributed, 2. Samples drawn from the population should be random, Cases of the samples should be independent. Student t test ( two tailed, independent) has been used to find the significance of study parameters on continuous scale between two groups (Inter group analysis) on metric parameters. Chi-square/ Fisher Exact test has been used to find the significance of study parameters on categorical scale between two or more groups.
+ Suggestive significance (P value: 0.05 < P<0.10)
* Moderately significant ( P value: 0.01 < P ≤ 0.05)
** Strongly significant (P value: P ≤ 0.01)
The Statistical software namely SAS 9.2, SPSS 15.0, Stata 10.1, MedCalc 9.0.1 ,Systat 12.0 and R environment ver. 2.11.1 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables etc.
Results
The demographic profile were comparable and statistically similar in both the groups (Table 1).
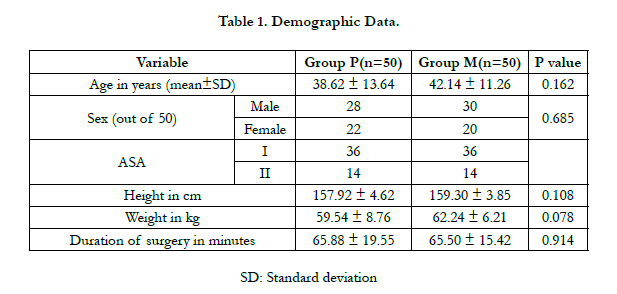

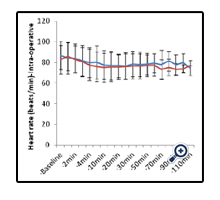
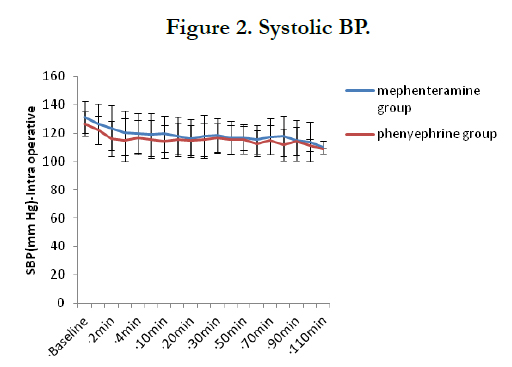
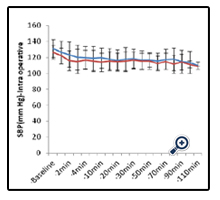
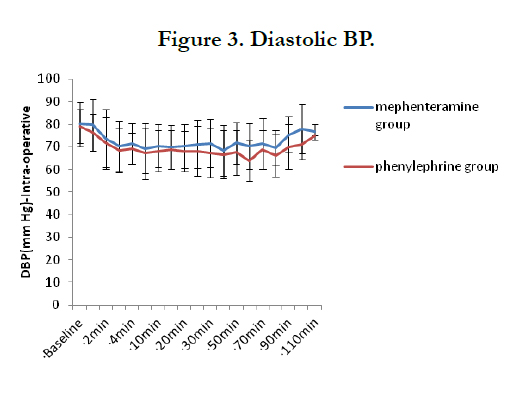
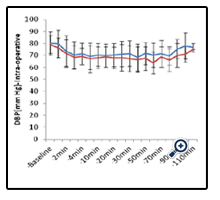
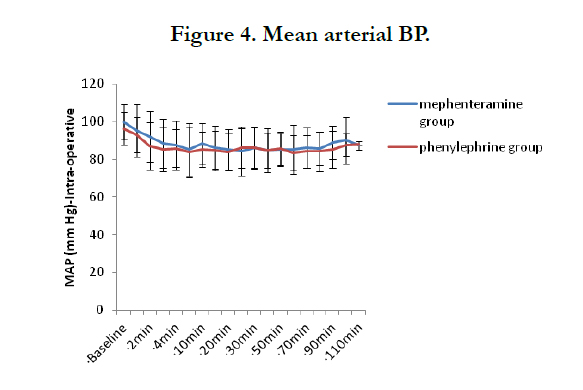
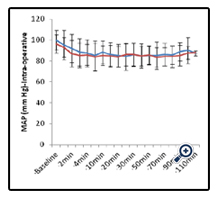
Intraoperative heart rate, systolic, diastolic and mean BP are depicted in the graphs below and are comparable and statistically similar (Figure 1-4).
The incidence of hypotension is similar in both the groups (Table 2).
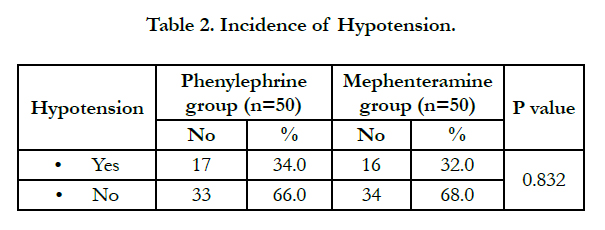
As depicted in Table 2, hypotension was observed in 17 patients (34%) in group P and 16 patients in group M. One episode of hypotension was observed in 8 patients (16%) in group P, 12 patients (24%) in group M. 7 patients (14%) in group P, 4 patients (8%) in group M had two episodes of hypotension. Which shows BP is maintained persistently high in Group M (Table 3).
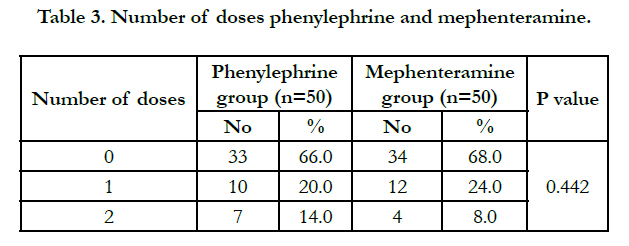
As depicted by Table 3, the average number of drug doses required to treat hypotension in the these groups were 1.41 in group P as compared to 1.25 group M respectively and statistically insignificant.
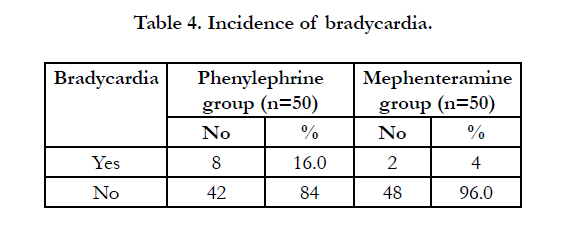
Incidence of bradycardia was more with phenylephrine group which was noted after the phenylephrine dose was given. But this reflex bradycardia was easily treatable with atropine. As per results shown in Table 4, bradycardia was observed in 8 patients (16%) in group P, 2 patients (4%) in group M. Each episode of bradycardia was treated with intravenous bolus of 0.6 mg atropine (Table 4).
Discussion
Hypotension caused by subarachnoid block has been the subject of research for decades, and still remains an important clinical problem. The management of this problem has therefore become important and various methods are employed for the management of hypotension. Although fluid preloading is still widely used its place in the management of hypotension induced by spinal anaesthesia has been questioned. Vasopressors are nowadays becoming one of the mainstays of management of spinal hypotension. Prophylactic use of vasopressors, intramuscular and subcutaneous routes rule out the possibility of dose titration and may result in either inadequate treatment or, more seriously, hypertension [13].
Commonly used vasopressors are ephedrine, mephenteramine, and phenylephrine. Phenylephrine is synthetic catecholamine which is an alpha 1 agonist acting by direct effect alpha 1 receptors. Resulting venoconstriction is greater than arterial constriction [14]. The alpha- mediated vasoconstriction leads to increase in peripheral vascular resistance. The rise in blood pressure causes baroreceptor mediated reflex sinus bradycardia. Mephentermine is an indirect acting vasopressor whose pharmacological action largely results from endogenous release of catecholamines. It has positive inotropic and chronotropic effect at the sinoatrial node but this effect is usually overcome by increased vagal activity occurring as a reflex to increased blood pressure. Thus, heart rate may be increased, decreased or unchanged.
In our study phenylephrine(100mcg) and mephenteramine(6mg) were used as boluses and were equally effective to treat hypotension during spinal anaesthesia in infraumblical surgeries. Bradycardia was noted more in phenyleprine group after phenylephrine bolus but treatable with iv atropine.
Dr. Dinesh Sahu et al., [15] compared bolus of phenylephrine, ephedrine and mephentermine for maintenance of arterial pressure during spinal anaesthesia in caesarean section and concluded that the phenylephrine, ephedrine and mephentermine are effective in IV bolus form in maintenance of arterial pressure within 20% limit of baseline though phenylephrine has quicker peak effect of comparison to ephedrine & mephentermine and it causes reduction in heart rate, which may be advantageous in cardiac patients and patients in whom tachycardia is undesirable which is similar to our study.
Anilkumar Ganeshanavar et al., [16] compared bolus of phenylephrine, ephedrine and mephentermine for maintenance of arterial pressure during spinal anaesthesia and concluded that phenylephrine group had quicker control of blood pressure compared to the other two groups. However, as the time elapsed all drugs achieved comparable control of blood pressure. Phenylephrine showed reduction in heart rate which is similar to our study.
R Sharma et al., [17] compared bolus of phenylephrine and mephentermine for treatment of hypotension during spinal anesthesia and concluded that mephentermine should be avoided in patients in whom increased heart rate may be undesired and Phenylephrine seems to be a better choice for the treatment of hypotension during spinal anesthesia. In our study both were effective in treatment of hypotension during spinal anaesthesia.
Fauzia Shifaat et al., [8] compared bolus of ephedrine, mephentermine and phenylephrine for maintenance of blood pressure during spinal anaesthesia during spinal anaesthesia in infraumbilical and lower limb surgeries and concluded that intravenous bolus of mephentermine 10 mg is better at maintaining blood pressure during spinal anaesthesia in infraumbilical and lower limb surgeries than intravenous bolus of ephedrine 10 mg and phenylephrine 100 μg. But in our study both were effective in treatment of hypotension during spinal anaesthesia for infraumbilical surgeries and hypotension was controlled effectively with lesser dose of mephentermine (6mg).
Devender Dua et al., [18] compared bolus of phenylephrine, ephedrine and mephentermine for maintenance of arterial pressure during spinal anaesthesia and concluded that all three vasopressor effectively maintained arterial pressure within 20% limit of baseline value though phenylephrine maintained better in first 6min of bolus dose as compared to ephedrine and mephentermine which may be due to that, phenylephrine has peak effect within 1 min, whereas ephedrine has 2-5 min and mephentermine has 5 min which was similar to our study.
M Mohta et al., [19] compared the effects of intravenous infusions of phenylephrine and mephentermine on the prevention of maternal hypotension and neonatal outcome in patients receiving spinal anaesthesia for caesarean section and concluded that phenylephrine and mephentermine infusions are equally effective in preventing post spinal hypotension in patients undergoing caesarean section and are associated with a similar neonatal outcome.
Conclusion
We conclude that intravenous bolus of phenylephrine and mephentermine are both effectve at maintaining intraoperative blood pressure during spinal anaesthesia in infraumbilical surgeries but mephenteramine is better than phenylephrine in maintaining BP persistently high and has lesser incidence of bradycardia.
References
- Sigdel S, Shrestha A, Amatya R (2015) Prevention of Spinal Anesthesia Induced Hypotension in Elderly: Comparison of Prophylactic Atropine with Ephedrine. J Anesth Clin Res 6: 557.
- Carpenter RL, Caplan RA, Brown DL, Stephenson C, Wu R (1992) Incidence and risk factors for side effects of spinal anesthesia. Anesth. 76: 906- 916.
- Arndt JO, Bömer W, Krauth J, Marquardt B (1998) Incidence and time course of cardiovascular side effects during spinal anesthesia after prophylactic administration of intravenous fluids or vasoconstrictors. Anesth Analg 87(2): 347-354.
- Riley ET, Cohen SE, Rubenstein AJ, Flanagan B (1995) Prevention of hypotension after spinal anesthesia for caesarean section: six percent hetastarch versus lactated Ringer’s solution. Anesth Analg. 81 (4): 838-842.
- Carron M, Freo U, Innocente F, Veronese S, Pilati P, Jevtovic-Todorovic V, Ori C (2007) Recovery profiles of general anesthesia and spinal anesthesia for chemotherapeutic perfusion with circulatory block (stop-flow perfusion). Anesth Analg. 105(5): 1500-1503.
- Greene NM, Brull SJ (1993) The cardiovascular system. Physiology of spinal anaesthesia. (4th edn), Baltimore: Williams and Wilkins. 85: 85-199, 177- 181, 309- 343 and 357-380
- Fischer Sp, Bader AM, Sweitzer BJ, Miller RD Preoperative evaluation. (7th edn), Millers Anaesthesia, United States.
- Fauzia Shifaat , Sheikh Imran Syed I, Sudershan Gupta, QaziDanish, Hilal Ahmad Wani (2016) Comparison of ephedrine, mephentermine and phenylephrine for maintenance of blood pressure during spinal anaesthesia. Int J Med Res. 2(2): 51-58.
- Bernard Rosner (2000) Fundamentals of Biostatistics (5th Edn), Cengage Learning, Duxbury, USA.
- Robert H Riffenburg (2005) Statistics in Medicine. (2nd edn), Academic press.
- Sunder Rao PSS, Richard J (2006) An Introduction to Biostatistics, A manual for students in health sciences. (4th edn), New Delhi: Prentice hall of India.
- Suresh KP and Chandrasekhar S (2012) Sample Size estimation and Power analysis for Clinical research studies. Human Reproduction Science. 5(1): 7-13.
- Rolbin SH, Cole AFD, Hew EM, Pollard A, Virgint S (1982) Prophylactic intramuscular ephedrine before epidural anaesthesia for caesarean section: efficacy and actions on the fetus and newborn. Can Anaesth Soc J. 29(2): 148-153.
- Ayorinde BT, Buczkowski P, Shah, Buggy DJ (2001) Evaluation of preemptive intramuscular phenylephrine and ephedrine for reduction of spinal anaesthesia-induced hypotension during Caesarean section. Br J Anaesth. 86(3): 372-6.
- Dr. Dinesh Sahu, Dr. Dilip Kothari, Dr. Amrita Mehrotra (2003) Comparison of bolus phenylephrine, ephedrine and mephentermine for maintenance of arterial pressure during spinal anaesthesia in caesarean section – a clinical study. Anaesth. 47 (2): 125-128.
- Anilkumar Ganeshanavar, Ambi Uday S, Shettar Adarsh E, Koppal Ramesh, R Ravi (2011) Comparison of bolus Phenylephrine, Ephedrine and Mephentermine for maintenance of arterial pressure during spinal anaesthesia in caesarean section. Clinical and Diagnostic Research. 5(5): 948-952
- R Sharma, N Maitra, M Niyogi (2008) A Comparative Study of Bolus Phenylephrine and Mephentermine for Treatment of Hypotension during Spinal Anesthesia for Cesarean Section. The Internet Journal of Anesthesiology.19(2).
- Dua D, Jadliwala R, Gondalia D, Parmar V , Jain A (2014) Comparison of bolus phenylephrine, ephedrine and mephentermine for maintenance of arterial pressure during spinal anaesthesia in caesarean section. Int J Pharm Sci Res. 5(6): 2412 -17.
- M Mohta, S Sai Janani, AK Sethi, D Agarwal, A Tyagi (2010) Comparison of phenylephrine hydrochloride and mephentermine sulphate for prevention of post spinal hypotension. Anaesthesia. 65:(12) 1200–1205.





