Peri-Operative Inflammatory Cytokines in Plasma of the Elderly Correlate in Prospective Study with Postoperative Changes in Cognitive Test Scores
Kline R1,5*, Wong E1,5, Haile M1,5, Didehvar S1, Farber S1, Sacks-Zimmerman A4, Pirraglia E2,6, de Leon MJ2,6, Bekker A3
1 Department of Anesthesiology, Perioperative Care and Pain Medicine, The New York University School of Medicine, USA.
2 Department of Psychiatry, The New York University School of Medicine, USA.
3 Department of Anesthesiology Rutgers NJMS.
4 Department of Neurological Surgery, Weill Cornell Medical.
5 New York University School of Medicine, Center for Cognitive Neurology.
6 New York University School of Medicine, Center for Brain Health.
*Corresponding Author
Richard Kline (c/o Mony deLeon),
145 E. 32nd Street, 5th Floor, New York University School of Medicine,
NY, NY 10016 USA.
E-mail: rpk1@columbia.edu
Received: June 15, 2016; Accepted: August 09, 2016; Published: August 16, 2016
Citation: Kline R, Wong E, Haile M, Didehvar S, Farber S, et al., (2016) Peri-Operative Inflammatory Cytokines in Plasma of the Elderly Correlate in Prospective Study with Postoperative Changes in Cognitive Test Scores. Int J Anesth Res. 4(8), 313-321.DOI : dx.doi.org/10.19070/2332-2780-1600065
Copyright: Kline R© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution
and reproduction in any medium, provided the original author and source are credited.
Abstract
Increasingly, postoperative cognitive dysfunction (POCD) is recognized as a complication after surgery in the elderly; but it’s etiology remains unclear. Here we examine changes in cytokine levels during both the pre-operative and postoperative period, comparing them with long term variation in cognitive test scores.
Forty-one patients aged 65 and older undergoing major surgery with general anesthesia were recruited after written consent in this IRB approved study. Thirty went on to complete this prospective, non-interven-tional and non-randomized study. Plasma levels of cytokines Il-6, Il-8, Il-10, and TNF were determined using ELISA with MILLIPLEX Multi-Analyte Profiling (Billerica, MA). All subjects had neurocognitive tests pre-operatively and 6 months post-surgery, including Paragraph Recall Immediate and Delayed, Digit Span Forward (DSF) and Backward (DSB), and Trail Making A and B.
Spearman’s Rho and repeated measure rank analysis were used to examine the dependence of z score changes in cognitive tests (baseline versus 6 months) as a function of 3 cytokine time points (presurgical, post anesthesia care unit (PACU), and post-operative day one (POD1)).
A greater increase in PACU inflammatory burden correlated with a greater decline in performance on the DSB (IL6, IL8; r>-0.560; p<= 0.008). DSF changes correlated slightly better with pre-surgical cytokines, declining more with higher cytokines (IL6, r= -0.551, p=0.002; IL8, -0.468, 0.009). TNF, examining all 3 values, changed only slightly postoperatively, but still correlated with a decline in DSB (p=0.014).
Thus, cognitive performance, over 6 months post surgery, declines with elevated perioperative inflammation. Specific cytokines at specific perioperative times may impact specific cognitive functions, serving as diagnostics as well as contributing causation.
2.Abbreviations
3.Introduction
4.Methods
4.1.Subject population
4.2.Cognitive testing
4.3.Blood Sampling and Cytokine Data Collection
4.4.Statistical Analysis
5.Results & Discussion
5.1.Description of population
5.2.Relationship between inflammatory cytokines and perioperative time
5.3.Correlations of cytokines with point scores of cognitive tests
5.4.Cognitive z score changes and point scores of cytokines
5.5.Attention/working memory and Baseline Cytokine Score
5.6.Attention/memory and Estimated Peak Cytokine Z Scores
5.7.Comparison of Cognitive z Score Change with the 3 Time Points for Each Cytokine
5.8.Summary
5.9.Postoperative chronology
5.10.Digit Span, Hippocampus and Inflammation
5.11.Does direct surgical trauma cause POCD ?
5.12.Does presence of activated microglia in the elderly produce a more reactive systemic inflammation?
6.Conclusion
7.Ethics Approval and Consent to Participate
8.Acknowledgements
9.References
Keywords
Surgery; Cytokines; Inflammation; Cognitive Tests; Perioperative; Cognitive Dysfunction.
Abbreviations
ADNI: Alzheimer’s Disease Neuroimaging; BMI: Body Mass Index; CRP: C-Reactive Protein; DSB: Digit Span Backward ; DSF: Digit Span Forward; IL: Interleukin; IRB: Institutional Review Board; LPS: Lipopolysaccharide; MCI: Mild Cognitive Impairment; MCP 1: Monocyte Chemotactic Protein 1; MHC: Major Histocompatibility Class; MMSE: Mini-Mental State Exam; PACU: Post Anesthesia Care Unit; POCD: Postoperative Cognitive Dysfunction; POD1: Postoperative Day One; SD: Standard Deviation; TNFa: Tumor Necrosis Factor Alpha.
Introduction
Post-operative cognitive dysfunction (POCD) is a prevalent and debilitating post-operative complication [1-3]. It is defined as the relative deterioration of intellectual/cognitive capacity in domains such as working memory, attention, language comprehension and social integration following surgery. Moller et al., noted that POCD was present in 25.8% of patients over the age of 60 at one week post-operatively and in 9.9% of patients at 3 months postoperatively [1]. Therefore, POCD presents itself as a significant challenge for the perioperative management of an increasingly elderly patient population.
The pathophysiology of POCD is poorly understood. Surgical trauma results in the activation of the innate immune system leading to the release of inflammatory mediators. These can modulate the central nervous system, resulting in cognitive impairment in the weeks and months following surgery [4]. Particular attention has been paid to the examination of postoperative cytokine expression as it correlates with surgical complications [5].
Presurgical cytokine levels [6, 7] as well as the magnitude of cytokine elevations due to evoked cytokine release [8] have been identified as potential important indicators of future cognitive function. The magnitude and persistence of the elevation can be a function of, among other things: intraoperative medications, whereby dexmedetomidine was shown to significantly reduce post-operative peak interleukin 10 (IL-10) [9]; or patient cognitive health [8], whereby patients with preoperatively described impaired mental status had increased levels of IL-6, IL-8 and IL-10 postoperatively. Analytes whose blood levels have been reported to change include: IL-1β, IL-6, IL-8, IL-10, monocyte chemotactic protein one (MCP-1), c-reactive protein (CRP) and tumor necrosis factor alpha (TNF-α In aged rats, there is an exacerbation of the impact of partial hepatectomy [10] leading to greater up-regulation of post-operative IL-1β and IL-6 expression, and to more cognitive impairment than in younger rats; thus associating surgical trauma, POCD and age.
In a study on healthy, middle aged patients, free of dementia, surgical injury or age related cognitive loss [11], plasma IL-6 levels were found to be inversely proportional to hippocampal grey matter volume, where-hippocampal atrophy is associated with loss of cognitive performance. In a related study on over 500 middle aged subjects, cognitive change showed an inverse relationship with plasma IL-6 [12] as predicted.
In our study, we hypothesized that the degree of inflammation measured preoperatively as elevated cytokines, or postoperatively as the incremental magnitude or elevated level of inflammatory cytokines, could contribute to the magnitude of cognitive decline measured 6 months after surgery. Confirming such a relationship and defining key elements could help to stratify prospective surgical patients with cognitive risk, as well as to provide an opportunity to modify such risk through interventions.
Methods
We received approval for this study by the New York University Langone Medical Center Institutional Review Board (IRB; FWA #00004952; compliant with Declaration of Helsinki), and initially enrolled 41 patients aged 65 and older who were scheduled to undergo spinal surgery, joint replacement, and other major surgeries under general anesthesia. Five enrolled patients were shortly lost to follow up and removed from analysis, leaving 36 participants, of whom 30 went on to complete this prospective, non-randomized study (IRB #H08658). Participants were selected in the pre-admission testing suite or by referral from participating surgeons offices several weeks prior to surgery. They were entered into the study sequentially, without randomization, if they passed inclusion/exclusion criteria. Fluency in written and verbal English was mandated, since all cognitive testing was in English. Written informed consent was required of all subjects. Moreover, written informed consent was obtained from all subjects. However, no identifiable data will be reported. Exclusion criteria included patients undergoing emergent procedures, extant dementia, preexisting psychological disorders and concurrent participation in another clinical study. Protocols for surgical or anesthetic care were not altered by participation in this study. Since this study was started in 2007 (prior to current registration requirements) and had no randomization, no therapeutic or greater than minimal risk interventions associated with the experimental component, it is compliant with human subject regulations even though not registered. It is not a human clinical trial.
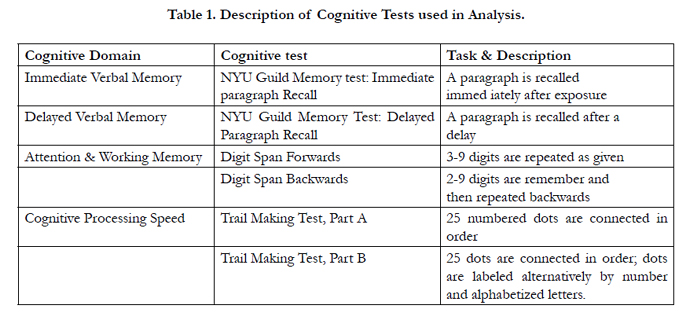
Subjects were asked to complete neurocognitive tests once preoperatively and again 6 months post-operatively. Tests included the following: Paragraph Recall Immediate and Delayed, Digit Span Forward (DSF) and Backward (DSB), and Trail Making A and B. Table 1 gives descriptions of these tests. These scores were trans-formed using regression based norms (age, gender, baseline score, time to followup) derived based on data from the NYU Center for Brain Health.

Preceding the induction of general anesthesia, blood samples were drawn for examining levels of cytokines, including TNF , and IL-6, IL-8, and IL-10. The first sample was the preoperative baseline. The two postoperative samples occurred in the PACU and on postoperative day 1 (POD1). Samples were acquired prior to the infusion of fluids in the PACU and on POD1. Within 30 minutes of collection, the samples were centrifuged and the plasma was isolated and stored at minus 70°C.
Plasma cytokines were evaluated with Luminex multiplexed bead-based immunoassays for inflammatory mediators. Multianalyte profiling was conducted on the Luminex-200 system and the XMAP Platform (Luminex Corporation, Billerica Mass). Calibration microspheres were provided for classification. Reporter readings and sheath fluid were purchased from Luminex Corporation. Analysis of obtained fluorescence data was provided from Beadview software. Analysis was conducted per manufacturer protocols with 1 pg/ml the lower limit of cytokine detection boundaries. The lower limits of detection for specific protein standards were acquired through software based extrapolation of diluted standards.
Z scores for the cognitive performances were determined against normative data, including a difference score of the z values. The z diff score was calculated by the following formula: (actual score – normative group score)/SD of the normative group, where SD is standard deviation. Standardized change was calcu-lated by (follow up z score–baseline z score). When confounds were considered, the expected change was calculated by a regression equation based on change score norms = constant + β1*age + β2*education + β3*sex + β4*baseline z score + β5*confound. The regression equation was derived from a robust sample of cognitively normal elderly subjects [13].
We examined correlation relationships between variables with the non-parametric Spearman’s Rho. Results were presented as correlation coefficient (r) and significance (p). These correlations were used to assess the relationships within and across time points, and between different cytokines. We also examined the relationships between cytokines at different time points and changes in values of cognitive scores between presurgical baseline and 6 months postsurgery. We initially used categorical diagnostics obtained by grouping the cognitive tests and generating z scores, as well as forming composite cytokine values; but later decided that better statistical analysis could be done examining continuous values of individual cognitive test scores and cytokine levels. Both approaches gave similar findings in terms of the impact of elevated cytokines on cognitive performance. For example, the group with the worst cognitive prognosis overlapped the group with highest cytokine values. However, we report below the findings using continuous values.
To utilize all the data for each cytokine (all 3 samples) – we employed repeated measures ANOVA where dependent variable ( SPSS ‘factor’) was the particular cytokine value over all 3 visits, and the change in individual cognitive test scores were covariates. Due to the failure to satisfy normality requirements, we used a non-parametric version of repeated measures. Cytokine values for all 3 time points were grouped together and ranked. The actual values were then replaced with the ranks [14] and examined with repeated measures ANOVA (N=20 for this analysis, since no missing data was allowed). A second method was also used for confirmation that at least 1 cytokine related to each digit span test. This method relied on calculating Pillai’s trace on the ranks within each variable [15].
For these rank calculations, we categorized the change in DSF and DSB into 3 equal size groups based on the size of the score change, and then tested the significance of this tertiary cofactor. This allowed us to visualize the relationships by plotting the mean rank of the cytokine value for each group (y axis) versus the time point (x axis), with each group in the categorical having its own line (for the small, medium and large z score change).
Multiple comparison corrections were performed using a sequentially rejective multiple test procedure [16]. The first comparison divided alpha (0.05) by N (the number of comparisons tested) and applied the new probability to the smallest obtained p value. The next largest p value was tested against alpha divided by N-1 etc.
In examining all pair wise correlations of cytokine measurements (n=66) there were 17 uncorrected p values at p = 0.000; so there remain many significant correlations after these corrections. The fact that about half of the correlations are significant at p < 0.05 (uncorrected), and as much as a quarter significant at p < 0.01 (uncorrected) implies that these are not all false positives, since this result would be unlikely by chance. Many of the correlations are informative, even if not strictly significant when corrected, and can be used to formulate hypotheses for modeling the cytokine interactions and how the inflammatory pathways respond.
The repeated measure analysis was used to validate the relation between cognitive change and cytokines, in the face of these corrections. Finally, p < 0.05 was considered statistically significant for all tests. Statistical ‘p’ values shown are uncorrected unless otherwise indicated.
Results & Discussion
The population was divided between males (n=16) and females (n=14), with average age in years of 73.5 (+7.4 std), mini-mental score of 28.8 (+1.6) and BMI of 26.6 (+6.1). Age, MMSE and BMI were the same by gender. Only years of education differed (p = 0.046; F, 15.3 + 3.0; M, 17.54 + 2.3 ).
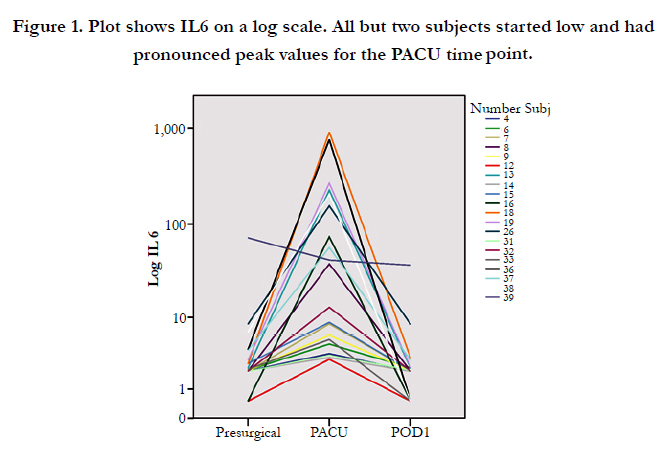
All the cytokines, except TNF (see below) show a characteristic spike in plasma activity in the PACU, followed by a drop towards presurgical values by POD1. See Figure 1 for individual plots of IL6 trajectories superimposed over all subjects. Elevations can exceed 2 orders of magnitude.
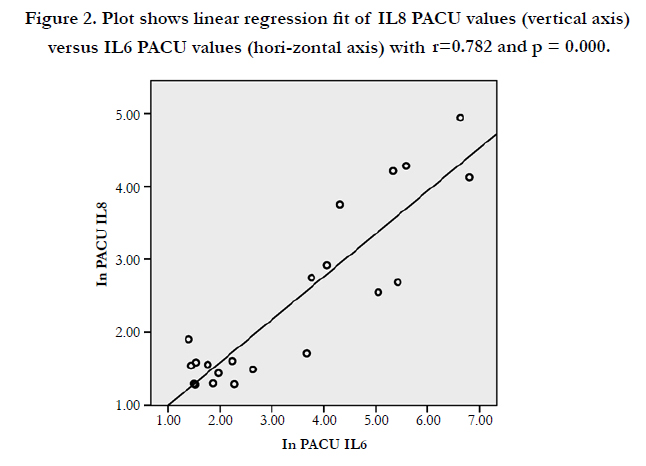
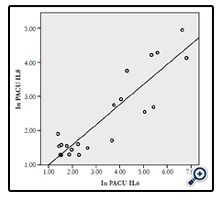
There is a strong relationship between values of all the cytokines (IL6, 8, and 10; TNF ) taken at the same visit. Examining IL-8, the cytokine whose values showed the best correlation across visits, there is a good correlation between the first (presurgical) and last (POD 1) measurement (r=0.676; p = 0.000), where the cytokine has almost returned to baseline values. There is also a good correlation between the PACU measurement (the postoperative spike in level) and the presurgical measurement for IL8 (r = 0.783; p = 0.000). The PACU values for the various cytokines correlate well with each other (see Figure 2: PACU IL6 plotted vs PACU IL8; r=0.782, p=0.000). PACU values of all cytokines correlate well with each other; i.e., PACU values for IL-6, 8 and 10, and TNF for all pairs have r > 0.695 and p=0.000.
There were also very good correlations between all presurgical values of the different cytokines (p < 0.005; with the exception of IL6 and TNF p = 0.026). POD1 values of cytokines IL8, IL10 and TNF strongly correlate (r >= 0.596; p <= 0.001) with each other; but not with POD1 of IL6. There is strong correlation between pre-surgical and POD1 values for each cytokine (r > 0.490; p < 0.001), as well as between cytokines comparing these time points (with the exception of IL6). In sum there are many strong correlations for cytokines across visits or by visit across cytokines.
Digit span test values (Forward or Backward) correlated with cytokines only by way of the digit span 6 month scores. Some cytokine point values did show significant correlation with 6 month digit span point values, especially PACU IL6 and IL8. The only cognitive point scores to correlate with cytokine values were the 6 month DSF or DSB. For example, 6 month DSF correlated with presurgical IL6 (r = -0.423; p = 0.020), IL8 (-0.417; 0.022), IL10 (-0.445; 0.014); and, PACU IL6 (-0.634; 0.002). DSB (6 month) correlated with presurgical IL10 (-0.377, 0.040), PACU IL6 (-0.734, 0.000), and IL8 (-0.582, 0.006). DSF at 6 months correlated with POD1 IL8 (-0.398, 0.040); and DSB at 6 mos correlated with POD1 IL8 (-0.497, 0.008), IL10 (-0.390, 0.044), and TNF (-0.450, 0.019). Both IL6 PACU comparisons would survive correction.
In looking at point values of cognitive scores and cytokine measurements, there were no Trails A or B values (either presurgical or POD180) which correlated with any cytokine values. Among the paragraph tests, only baseline paragraph delayed scores correlated with point cytokine values (presurgical IL8, PACU IL8, IL10 and TNF p<0.05; but the significance of these scores would not survive correction).
Based on the above analysis, it appears that the 6 month cognitive score correlations with cytokine values were to a large extent responsible for the cytokine point values correlating with the cognitive score changes from baseline to 6 months. The most significant and numerous correlations were between DSF and DSB z difference values and cytokines IL6 and IL8, where the pre-surgery and POD1 values tended to correlate well with DSF, and the PACU value (“peak” post surgical) correlated with DSB. There were no correlations between the difference in z scores of Trails A or B and any cytokine values. Among the paragraph scores, only the z difference of the immediate paragraph recall scores correlated with any point cytokine values (IL6; r = 0.411, p=0.024), but this did not survive correction. Therefore,further analysis was only for the DSF and DSB cognitive tests scores.
Detailed analysis showed that an elevated preoperative inflammatory burden was associated with a greater decline in performance on the Digit Span Forward (DSF) test (a measure of attention) at 6 months. Z score differences in DSF for presurgical Il-6, Il-8 and Il-10 separately were: -0.551 (p=0.002), -0.468 (p=0.009), and -0.457 (p=0.011), where IL6 is significant after multiple comparison correction, and the latter two show trends post correction.
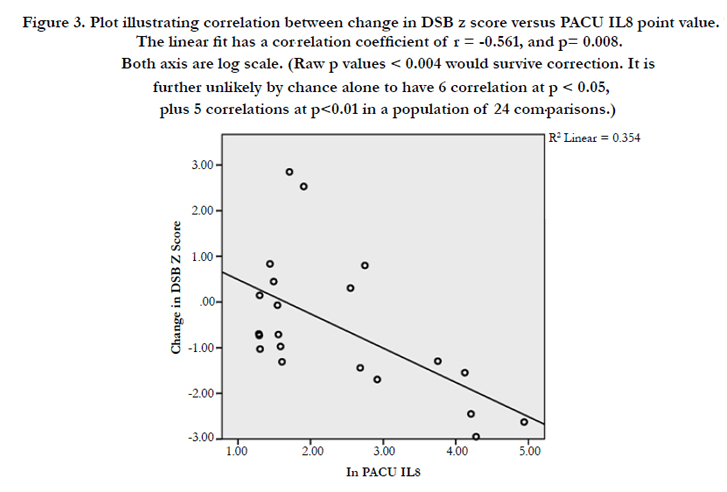
The post-surgical cytokine response also had an apparent relationship with cognitive performance. Particularly, the digit span backwards (DSB) test score change correlated with the estimated “peak” cytokine re-sponse for both IL6 and IL8. Correlation coefficients (and p values) for IL6 and IL8 versus DSB change were: -0.595 (p=0.004) and -0.561 (p=0.008). Figure 3 shows the relationship between DSB changes and the PACU values of IL8. DSB testing entails a more complex task than DSF, since digit order must be reversed while holding the list in memory. Thus DSB is a measure of attention, short term and working memory.
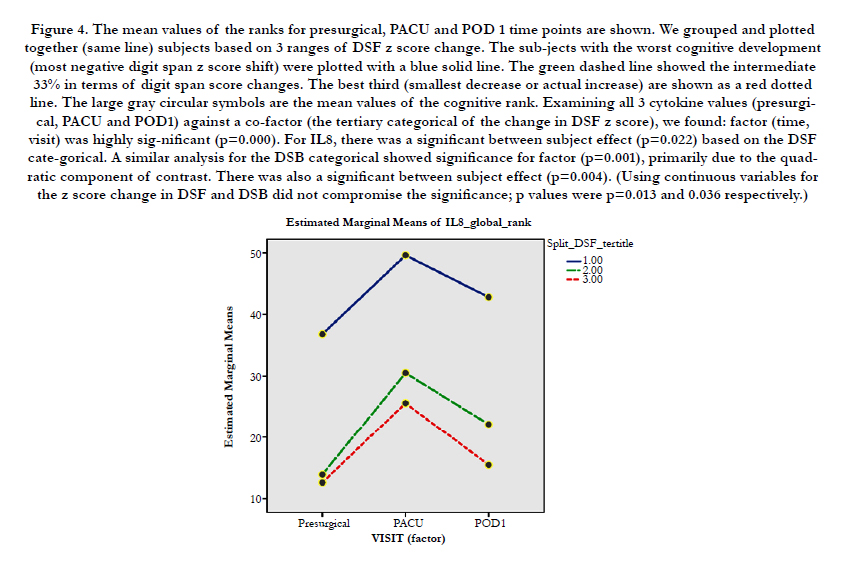
We combined the temporal evolution of the perioperative cytokine changes with the cognitive score changes for each patient (see plot, Figure 4). The subjects with the greatest loss in digit span backwards performance had the largest IL8 peak for the PACU measurement. We statistically tested this result using repeated measures analysis, where visit (time of cytokine measurement) was the 3 value factor, cytokine was the dependent variable and amount of DSB or DSF shift (as a categorical) was the cofactor. The purpose of this analysis was to enhance the power of the cytokine predictions by using all 3 values while eliminating some of the multiple comparison issues.
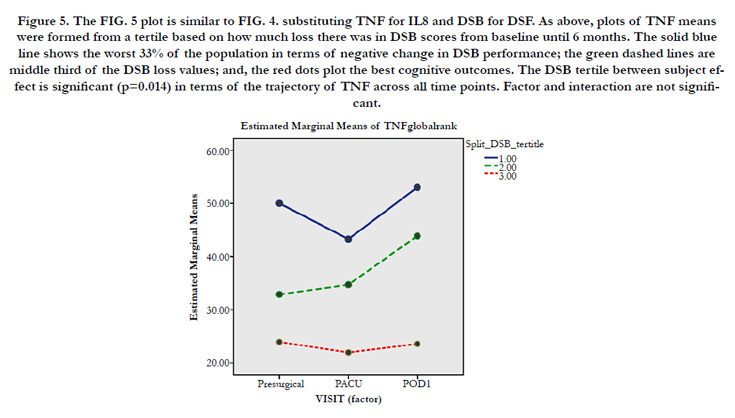
Using rank based repeated measure ANOVA, the categorical describing the magnitude of the change in digit span scores were significant for IL8 (see caption). Furthermore, factor was significant implying that cytokines changed with visit (p=0.000). Likewise, TNF was significantly dependent on DSB (p<0.03). However, factor was not significant for TNF implying that this cytokine did not change over time for each subject. Plots show cytokines over all 3 time points, indicating the different values of the z score categorical with different lines (See Figure 5). Due to the significant relationship for both IL8 and TNF, with both DSF and DSB, it is sug-gested that the entire trajectory of the cytokines is related to the impact on cognition. For IL6 (not shown), only the pre and PACU values (but not POD1) had a significant relationship to cognitive change. (But visit (factor) was highly significant (p=0.000) for IL6 as could be expected from Figure 1).
Our results show that perioperative values of cytokine concentrations, primarily IL-6 and IL-8, and to a lesser extent TNF and IL-10, correlate with changes in attention and working memory (as measured by DSF and DSB) post-operatively. This was consistent with our hypothesis that greater pre-operative levels of inflammation would lead to poorer cognitive function post-operatively. Interestingly, the strongest correlations occurred between the presurgical cytokine values and the change in digit span forward. On the other hand, the elevated values of cytokines occurring immediately postoperatively (in the PACU) tended to correlate with the change in the digit span backwards scores. There was no direct correlation between the DSF and DSB scores, and either IL6 or IL8 at baseline. Finally, TNF, which showed much less change in the perioperative period, still correlated with digit span forward and backward changes in the repeated measures analysis.
The DSF test has been implicated in postoperative changes either by itself [17] or in a composite of several other executive function tests [18]. In the study of the dependence of cognitive changes on variation in IL-6 blood levels, healthy middle age subjects showed decreased performance with increased IL-6, but primarily for executive function tests. We have presented these detailed relationships to motivate future study by suggesting that: 1) Several different cytokines correlate with changes in cognitive function; and, 2) The particular time (perioperative phase) of cytokine change was significant in terms of the actual tests affected.
It is notable that elevation of different cytokines can indicate different etiologies of inflammatory cause, as well as a difference in potential outcomes. The elevation of one class of inflammatory cytokine may be induced by an entirely separate mechanism when compared to another. In one study comparing septic shock and non-septic shock [19], it was notable that both non-septic and septic shock patients had elevated IL-6 levels, but IL-8 was elevated in the septic patients only. Our findings of similarities and differences in terms of IL6 and IL8 behavior is generally consistent with this notion.
Cytokine makeup of a patient can have predictive value [20]. TNF levels were measured in septic patients, which revealed a 73% (8/11) mortality rate for patients found to be TNF positive, compared to a 34% (11/32) mortality rate for TNF negative patients. The study was able to demonstrate that sepsis is accompanied by detectable levels of TNF in 25% of cases, and that mortality amongst TNF-positive patients was nearly twice that compared to TNF-negative patients. Another study evaluating IL- 6, IL-8, CRP, and TNF-alpha amongst centenarians demonstrated baseline TNF- as an independent prognostic marker for mortality in the respective patient population, as was CRP prognostic in the absence of TNF elevation [21].
The exact kinetics of the cytokines should not be over interpreted; since they are measured downstream in the systemic circulation, were released from different cell groups in different locations, and were lost to the circulation at different rates and by different mechanisms. For example, IL-6 is recognized as a product of some astrocytoma and glioma cell lines when stimulated by IL- 1B [22]. Its presence in plasma could either be a product of systemic inflammatory cells, or a pathological increase in blood brain barrier permeability resulting from major surgery [23]. Thus relative permeability of the blood brain barrier could affect blood levels of all cytokines released intracortically and lead to increased correlation of cytokine changes in the PACU. Further more, the PACU value presumably has more complicated dependence on other factors than the baseline value, since it depends on baseline, the amount released due to surgery, the reuptake/washout process, and the kinetics of these processes.
It is important to note that we published on this same population that a reduced cognitive performance was still detected 6 months after surgery in some patients. Other patients saw no change or improvement by this time [24]. We also have reported on surgical patients identified in a retrospective study from the ADNI database that there was atrophy in both hippocampal and total gray matter volume as measured during the 6 month interval which included the surgery. The perioperative atrophy in the surgical population exceeded that in non-surgical patients from this same database [18]. Unfortunately, there is no imaging component in this study, but the previous study suggests that a prolonged impact of surgery is plausible.
The permanence of these effects are obviously important. If the cognitive defects are no longer detectable at 1 year after being detected earlier [25], is this because the disruptive factor decayed (dissipation of inflammation) or because neural assets were restored (plasticity)? In an analysis of 20 joint surgery patients identified in the Alzheimer’s Neuroimaging Database (ADNI;[26]), the surgery related atrophy, which developed over the 6 month interval including the surgery, was seen to resolve during the 2nd 6 month interval (the 6 month interval following the surgical interval). Thus, by one year, cortical and hippocampal volumes were not different than baseline in these joint replacement/repair patients (although not in all surgical patients). This suggests that neural plasticity may be a factor in countering POCD related atrophy. However, the initial atrophy could still affect cognition months later even with plasticity since restoration of neuronal volume doesn’t necessarily mean restoration of cognitive function.
Studies using animal models also promote the idea of reversibility of post-operative cognitive dysfunction, only over a shorter time span [10]. It is promising to consider acute post-operative cognitive dysfunction to be potentially reversible, consistent with evidence of the plastic and regenerative nature of the brain [27].
It is also notable that our study did not find a correlation between cytokine concentration and the other components of the neuropsychological battery, including the tests for immediate verbal memory, delayed verbal memory, or motor processing speed, listed above. However, these results are still consistent with current research trends, as it is widely recognized that the hippocampus serves as a center for attention and short term memory processing [28]; and, there is much evidence that activation of the peripheral immune system results in a robust increase in inflammatory cytokine mRNA levels in hippocampaltissue [29, 30]. Studies have identified IL-6 as a key mediator of hippocampal grey matter volume loss and shown that higher levels of peripheral IL-6 usually associated with inflammation negatively affect memory and learning [11, 12]. Animal studies have found mechanistic links between inflammation and cognitive decline, with specific focus on microglia and the hippocampus responding to peripheral stimulation and surgery [31-33]. Studies also point to inflammation as having complex, often contradictory effects on neuroplasticity, with both the introduction and subsiding of inflammatory cytokines being important in facilitating cortical plasticity [34-36].
Our study tries to make a distinction between post-operative cognitive changes due to direct surgical trauma, and changes that result from the pre-existing inflammation being further exacerbated. Recall the different cognitive effects resulting from elevation of presurgical cytokines versus those correlating with immediately postsurgical release.
Previous studies have pointed to surgical trauma as the major contributor to cognitive impairment, mainly from peripheral inflammation activating inflammatory processes in the central nervous system. Yet it should also be noted that surgeries which frequently decrease pain and inflammation, like joint replacement and coronary bypass surgery have been associated with both cognitive improvement and a greater quality of life [27]. Many researchers assume the brain to retain a lifelong plasticity and capacity to regenerate against physiological duress [37, 38]. With the resolution of pain through successful surgery, neuroanatomical repletion of lost volume may be a possibility. Therefore, it is our hypothesis that analyzing the inflammatory processes associated with both surgical trauma and pre-operative state is optimal in terms of predicting surgical outcomes. Overreliance on static baseline levels of plasma analytes, rather than the dynamic changes occurring after a large stimulus - like surgery - may miss important elements involved in the cellular signaling pathway.
Levels of inflammation are notably higher in the elderly [39]. Age has been identified as one of the most important factors increasing POCD risk [1]. Increased age alone is associated with an increase in cytokines [40]. Another factor associated with POCD is pre-existing cognitive impairment [25], usually associated with aging. Patients who were found to have pre-operative mild cognitive impairment (MCI) had a greater postoperative decline in performance, when compared to surgical patients without MCI [17, 18].
Elderly mice have a hyper-reactive pro-inflammatory response by microglia surrounding the hippocampus, and show higher expression of major histocompatibility (MHC) class II, a marker of microglia, in their brains as compared to young mice [41]. Mice treated with lipopolysaccharide (LPS) and evaluated for cytokine mRNA levels within surrounding hippocampal tissue [42] showed not only higher cytokine mRNA levels in the CNS hippocampal region, but also increased microglia staining in the aged versus the young mice.
Conclusion
Thus, cognitive performance, measured by its change at 6 months post surgery, correlates with periopera-tive inflammation per changes in plasma levels of 4 cytokines. Specific cytokines at specific perioperative times may impact specific cognitive function, serving as diagnostics as well as contributing causation.
Ethics Approval and Consent to Participate
This described study was approved by the NYU Medical School IRB OHRP FWA #00004952 in compliance with the Declaration of Helsinki. Written Informed Consent was required of all subjects and all subjects did in fact give written consent. No identifiable subject information is presented. The study, NYU IRB #H08-658, is not a clinical trial since there are no therapeutic interventions, it is not randomized, and the research component is minimal risk.
Acknowledgements
This study was supported by NIH/NIA grants AG035137, AG032554, AG022374, AG13616, AG12101, AG08051, which support the participation of Mony de Leon and Elizabeth Pirraglia.
References
- Moller JT, Cluitmans P, Rasmussen LS, Houx P, Rasmussen H, et al., (1998) Long-term postoperative cognitive dysfunction in the elderly ISPOCD1 study. ISPOCD investigators. International Study of Post-Operative Cognitive Dysfunction. Lancet 351(9106): 857-861.
- Newman S, Stygall J, Hirani S, Shaefi S, Maze M: Anesthesiology (2007) Postoperative cognitive dysfunction after noncardiac surgery: a systematic review. 106(3):572-590.
- Rohan D, Buggy DJ, Crowley S, Ling FK, Gallagher H et al.,(2005) Increased incidence of postoperative cognitive dysfunction 24 hr after minor surgery in the elderly. Can J Anaesth. 52(2):137-142.
- Buchanan JB, Sparkman NL, Chen J, Johnson Rw (2008) Cognitive and neuroinflammatory consequences of mild repeated stress are exacerbated in aged mice. Psychoneuroendocrinology. 33(6):755-765.
- Baigrie RJ, Lamont PM, Kwiatkowski D, Dallman MJ, Morris PJ (1992) Systemic cytokine response after major surgery. Br J Surg. 79(8):757-760.
- Hirsch J, Vacas S, Meckler G, Newman S, Kramer J, et al.,(2014) Perioperative cytokine patterns in CSF and Plasma during and after knee replacement surgery. Anesth Analg 118(5S): S-133.
- Haile M, Kline R, Sachs A, Pirraglia E, Didehvar S, et al. (2013) Pre-operative inflammatory burden in the elderly increases the risk of developing postoperative cognitive dysfunction. Anesth Analg 116(5S): 196.
- Beloosesky Y, Hendel D, Weiss A, Hershkovitz A, Grinblat J et al.,(2007) Cytokines and C-reactive protein production in hip-fracture-operated elderly patients. J Gerontol A Biol Sci Med Sci. 62(4):420-426.
- Alex Bekker, Michael Haile, Richard Kline, Sorosch Didehvar,Ramesh Babu (2013) The effect of intraoperative infusion of dexmedetomidine on the quality of recovery after major spinal surgery. J Neurosurg Anesthesiol. 25(1):16-24.
- Cao XZ1, Ma H, Wang JK, Liu F, Wu BY et al., (2010) Postoperative cognitive deficits and neuroinflammation in the hippocampus triggered by surgical trauma are exacerbated in aged rats. Progress in neuro-psychopharmacology & biological psychiatry. 34(8):1426-1432.
- Marsland AL, Gianaros PJ, Abramowitch SM, Manuck SB, Hariri AR (2008) Interleukin-6 covaries inversely with hippocampal grey matter volume in middle-aged adults. Biol Psychiatry. 64(6):484-490.
- Marsland AL, Petersen KL, Sathanoori R, Muldoon MF, Neumann SA SB (2006) Interleukin-6 covaries inversely with cognitive performance among middle-aged community volunteers. Psychosomatic medicine, 68(6):895-903.
- De Santi S, Pirraglia E, Barr W, Babb J, Williams S, et al (2008) Robust and conventional neuropsychological norms: diagnosis and prediction of agerelated cognitive decline. Neuropsychology, 22(4):469-484.
- Thompson GL (1991) A Unified Apporach to Rank Tests for Multivariate and Repeated Measures Designs. Journal of the American Statistical Association. 86(414):410-419.
- Zwick R (1985) Nonparametric one-way multivariate analysis of variance: a computational approach based on the Pillai-Bartlett trace. Psychological bulletin. 97(1):148-152.
- Holm S (1979) A Simple sequentially Rejective Multiple test Procedure. Scandinavian Journal of Statistics. 6(2):65-70.
- Bekker A, Lee C, de Santi S, Pirraglia E, Zaslavsky A at el., (2010) Does mild cognitive impairment increase the risk of developing postoperative cognitive dysfunction. Am J Surg. 199(6):782-788.
- Kline RP, Pirraglia E, Cheng H, De Santi S, Li Y at el.,(2012) Surgery and brain atrophy in cognitively normal elderly subjects and subjects diagnosed with mild cognitive impairment. Anesthesiology. 116(3):603-612.
- Marty C, Misset B, Tamion F, Fitting C, Carlet Jat el., (1994) Circulating interleukin-8 concentrations in patients with multiple organ failure of septic and nonseptic origin. Crit Care Med. 22(4):673-679.
- Debets JM, Kampmeijer R, van der Linden MP, Buurman WA, van der Linden CJ (1989) Plasma tumor necrosis factor and mortality in critically ill septic patients. Crit Care Med. 17(6):489-494.
- Bruunsgaard H, Andersen-Ranberg K, Hjelmborg J, Pedersen BK, Jeune B (2003) Elevated levels of tumor necrosis factor alpha and mortality in centenarians. Am J Med. 115(4):278-283.
- Erta M, Quintana A, Hidalgo J: (2012) Interleukin-6, a major cytokine in the central nervous system. International journal of biological sciences. 8(9):1254-1266.
- Merino JG, Latour LL, Tso A, Lee KY, Kang DW at el.,(2013) Blood-brain barrier disruption after cardiac surgery. AJNR Am J Neuroradiol. 34(3):518- 523.
- Sacks A, Haile M, Pirraglia E, Farber E, Chu A, et al., (2012) PostOperative Cognitive Changes in the Elderly. American Academy of Clinical Neuropsychology, Proceedings,Meeting, Seattle Washington.
- Silbert B, Evered L, Scott DA, McMahon S, Choong P at el., (2015) Preexisting cognitive impairment is associated with postoperative cognitive dysfunction after hip joint replacement surgery. Anesthesiology. 122(6):1224-1234.
- Kline RP, Pirraglia E, Li Y, Haile M, de Leon JM, et al., (2012) Impact of Surgery Type On Postsurgical Changes in Cortical Volume. Anesthesiology(abstract) A021.
- Avidan MS, Benzinger TL (2012) Surgery and the plastic brain. Anesthesiology. 116(3):510-512.
- Anderson P, Morris R, Amaral D, Bliss T, O'Keefe, J (2007)Historical perspective: Proposed functions, biologicalcharacteristics, and neurobiological models of the hippocampus. (1st edn). Oxford University Press ,New York.
- Berg BM, Godbout JP, Chen J, Kelley KW, Johnson RW (2005) alpha-Tocopherol and selenium facilitate recovery from lipopolysaccharide-induced sickness in aged mice. J Nutr. 135(5):1157-1163.
- Laye S, Parnet P, Goujon E, Dantzer R (1994) Peripheral administration of lipopolysaccharide induces the expression of cytokine transcripts in the brain and pituitary of mice. Brain Res Mol Brain Res. 27(1):157-162.
- Katsuki H, Nakai S, Hirai Y, Akaji K, Kiso Y at el.,(2007) Postoperative impairment of cognitive function in rats: a possible role for cytokine-mediated inflammation in the hippocampus. Anesthesiology. 106(3):436-443.
- Katsuki H, Nakai S, Hirai Y, Akaji K, Kiso Y (1990) Interleukin-1 beta inhibits long-term potentiation in the CA3 region of mouse hippocampal slices. Eur J Pharmacol. 181(3):323-326.
- Bernardino L, Xapelli S, Silva AP, Jakobsen B, Poulsen FR at el.,(2005) Modulator effects of interleukin-1beta and tumor necrosis factor-alpha on AMPA-induced excitotoxicity in mouse organotypic hippocampal slice cultures. J Neurosc. 25(29):6734-6744.
- Greifzu F, Schmidt S, Schmidt KF, Kreikemeier K, Witte OW at el., (2011) Global impairment and therapeutic restoration of visual plasticity mechanisms after a localized cortical stroke. Proc Natl Acad Sci U S A.108(37):15450-15455.
- Suzuki S, Tanaka K, Suzuki N (2009) Ambivalent aspects of interleukin-6 in cerebral ischemia: inflammatory versus neurotrophic aspects. J Cereb Blood Flow Meta. 29(3):464-479.
- Liguz-Lecznar M, Kossut M(2013) Influence of inflammation on poststroke plasticity. Neural plasticity 2013. 2013:258582.
- Langer N, Hanggi J, Muller NA, Simmen HP, Jancke L (2012) Effects of limb immobilization on brain plasticity. Neurology . 78(3):182-188.
- Keller TA, Just MA (2009) Altering cortical connectivity: remediation-induced changes in the white matter of poor readers. Neuron 64(5):624-631.
- Krabbe KS, Pedersen M, Bruunsgaard H (2004) Inflammatory mediators in the elderly. Exp Gerontol.39(5):687-699.
- Ershler WB, Keller ET (2000) Age-associated increased interleukin-6 gene expression, late-life diseases, and frailty. Annu Rev Med. 51:245-270.
- Godbout JP, Chen J, Abraham J, Richwine AF, Berg BM at el., (2005) Exaggerated neuroinflammation and sickness behavior in aged mice following activation of the peripheral innate immune system. FASEB J.19(10):1329-1331.
- Chen J, Buchanan JB, Sparkman NL, Godbout JP, Freund GG at el., (2008) Neuroinflammation and disruption in working memory in aged mice after acute stimulation of the peripheral innate immune system. Brain Behav Immun. 22(3):301-311.





