Semisitting Position and Venous Air Embolism in Neurosurgical Patients with Patent Foramen Ovale: A Systematic Analysis
Kurnutala LN1*, Sandhu G2, Stoicea N2, Kinthala S3, Wei L4, Bergese SD2
1 Department of Anesthesiology, University of Mississippi Medical Center, Jackson, MS, USA.
2 Department of Anesthesiology, Wexner Medical Center, Ohio State University, Columbus, OH, USA.
3 Department of Anesthesiology, New York Methodist Hospital, Brooklyn, NY, USA.
4 Center for Biostatistics, Wexner Medical Center, Ohio State University, Columbus, OH, USA.
*Corresponding Author
Lakshmi N Kurnutala,
Assistant Professor and Director of Neuroanesthesia,
Department Of Anesthesiology, University of Mississippi Medical Center,
Jackson, MS. USA. 39216.
Tel: +1-601-984-5900
Fax: +1-601-984-5915
E-mail: lkurnutala@umc.edu
Received: June 08, 2016; Accepted: August 08, 2016; Published: August 11, 2016
Citation: Kurnutala LN, et al., (2016) Semisitting Position and Venous Air Embolism in Neurosurgical Patients with Patent Foramen Ovale: A Systematic Analysis. Int J Anesth Res. 4(8), 305-312.DOI : dx.doi.org/10.19070/2332-2780-1600064
Copyright: Kurnutala LN© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
The semisitting position (SSP) offers significant advantages for neurosurgeons but presents numerous challenges to anesthesiologists. One major concern is venous air embolism (VAE). The incidence of patent foramen ovale (PFO) is approximately 10-35%. Typically, PFO causes a left-to-right shunt, but there is also a possibility of paradoxical embolism. Patients who undergo sitting craniotomies are routinely evaluated using a preoperative transthoracic echocardiogram (TTE) or transesophageal echocardiogram (TEE). Even in the presence of a PFO, neurosurgeons frequently prefer to perform surgery in the SSP. The incidence of venous air embolism in the sitting position is 23-45%. However, the rate of clinically significant air embolism is significantly lower.
We conducted herein a systematic review of the incidence rates of PFO, venous air embolism, and complications in patients undergoing semisitting neurosurgical procedures. According to our analysis, the incidence of VAE was similar in both unknown and known PFO status patients (23.5% vs. 24.5%; p = 0.88) undergoing semisitting neurosurgical procedures. Other complications, such as hypotension, MI, stroke and perioperative deaths, could not be compared between the two groups due to inadequate power.
However, there is a lack of level A evidence from currently available observational studies. Definitive evidence-based recommendations and guidelines based on well-designed studies are required to address this problem.
2.Abbreviations
3.Introduction
3.1.Primary Objective
4.Methods
4.1.Literature Search
4.2.Inclusion and Exclusion Criteria
4.3.Data Extraction and Analysis
4.4.Quality Assessment and Statistical Analysis
5.Results
5.1.Flow of the Studies
5.2.Synthesis of Results
6.Discussion
7.Study Limitations
8.Conclusions
9.References
Keywords
Semisitting Position; Sitting Craniotomy; Posterior Cervical Spine Surgery; Venous Air Embolism; Patent Foramen Ovale; Paradoxical Air Embolism.
Abbreviations
CSS: Cervical Spine Surgery; MI: Myocardial Infarction; PAE: Paradoxical Air Embolism; PFO: Patent Foramen Ovale; PFS: Posterior Fossa Surgery (Brain); SP: Sitting Position; SSP: Semisitting Position; TCD: Transcranial Doppler; TEE: Transesophageal Echocardiogram; TTE: Transthoracic Echocardiogram; VAE: Venous Air Embolism.
Introduction
Proper positioning of a patient during surgery is an important determinant of the success of the procedure. Each type of position during surgery confers its own advantages and disadvantages, from the surgical and anesthetic points of view, but the final decision should serve the best interests of the patient. The benefits of, and alternatives to, semisitting craniotomy have been a source of contention since the early 1930s [1].This position offers excellent working conditions to the surgeon during performance of posterior fossa and cervical spine surgeries, but also presents significant challenges to anesthesiologists, of which the most important is venous air embolism (VAE).
The first recorded fatal VAE incidence was reported, in the sitting position (SP) during excision of a tumor on the right cheek, by John Barlow in 1830 [2]. In the context of neurosurgery, the SP has been a subject of interest for posterior fossa surgery (PFS) and posterior cervical spine surgery (CSS). A VAE occurs when atmospheric air is introduced into the systemic venous system; it represents a strictly iatrogenic complication. In the past, this medical condition was primarily associated with neurosurgical procedures conducted in the SP. More recently, VAE has also been observed during surgeries conducted in the prone and horizontal positions, and during invasive vascular procedures, high-pressure mechanical ventilation, thoracocentesis, hemodialysis, and in conjunction with penetrating and blunt chest trauma. The reported incidence of VAE occurring in the SSP is 0‒76% according to previous studies [3-40]. Patients with a patent foramen ovale (PFO) are at increased risk of PAE during semisitting position (SSP) craniotomy. The prevalence of PFO is approximately 25% (10‒35%) in the normal population, which rises to > 40% in cryptogenic stroke patient groups. PFO provokes a right-to-left shunt, which can in turn allow VAE migration, to the systematic arterial circulation, to cause a paradoxical air embolism (PAE) in certain patients [41,42]. Because of the high risk of VAE and PAE occurring in conjunction with PFO, neurosurgical patients being considered for semisitting craniotomies are routinely evaluated by either preoperative transthoracic echocardiogram (TTE), transesophageal echocardiogram (TEE) or transcranial Doppler (TCD).41-48 Diagnosis of a PFO is widely regarded as a contraindication for SSP craniotomy, yet certain neurosurgeons believe that the benefits of SSP outweigh the risks, even in the presence of a PFO [43-52].
Scant prospective data corroborating either position is available within the current literature, such that the issue of patient selection criteria for SSP craniotomy and posterior cervical spine surgery remains to be clarified.
The primary objective of this systematic review was to compare the incidence of VAE, and other complications, between patients with unknown and known PFO status undergoing neurosurgical procedures in the SSP.
Methods
The study protocol included literature-search strategies, inclusionexclusion criteria, incidence of VAE, presence of PFO, and methods of statistical analysis developed before performance of the systematic review. The protocol was prepared according to the Meta-Analysis of Observational Studies in Epidemiology [53], and Preferred Reporting Items for Systematic Reviews and Meta- Analyses, guidelines [54].
The following two groups were defined for the literature review: group I - studies of neurosurgeries performed in the SSP with unknown PFO status [15-40]; and group II - studies of neurosurgeries performed in the SSP with known PFO status [41-52] The Medline, Embase, and Cochrane Control Trial register databases were searched systematically for articles published between 1972 and April 2014, with no restriction on the publication language applied and using various combinations of the following keywords: semisitting craniotomy, sitting craniotomy, posterior cervical spine surgery, venous air embolism, patent foramen ovale, and paradoxical air embolism. All abstracts were screened according to the research question. Bibliographies identifying articles and reviews relevant to this field were also searched. Furthermore, hand searching of pertinent journals, for articles published during the previous 6 months, was undertaken. If any study generated multiple publications, the most-current report was used.
The inclusion criteria for group I were as follows: patients undergoing neurosurgical procedures in the SP or SSP, in studies with ≥ 15 patients reportedly experiencing episodes of VAE or PAE with unknown PFO status. For group II, the following inclusion criteria were applied: patients undergoing neurosurgical procedures in the SP or SSP, in studies with ≥ 15 patients reportedly experiencing episodes of VAE or PAE with known PFO status. The exclusion criteria for studies of either group were case report designs, studies with < 15 patients, animal studies, expert opinion reports, and unclear methodologies.
Database searches and data extraction were performed by two authors. The decision to include or exclude a study was made independently by both authors (L.N.K. and G.S.), with disagreements settled by the senior author (S.D.B.). The data from the included studies were tabulated into a standard Microsoft Excel® spreadsheet (Microsoft Office 2010, Microsoft Corp., Redmond, WA, USA). For groups I and II, the following data were recorded: name of author, publication year, type of study, sample size, mean age of subjects, neurosurgical procedure type, VAE incidence, method of detecting VAE, and special concerns of the study (e.g., PAE, hypotension, myocardial infarction [MI], stroke, death) during the procedures.
No randomized controlled studies with level A evidence were identified. Prospective, retrospective and combined studies were included in the analysis. (Evidence level B; American Academy of Family Physicians)[55]. In all studies, the outcomes were clearly defined and VAE incidence rate was the primary outcome. Given the nature of the studies available within the current literature, a traditional meta-analysis method, utilizing relative risk or odds ratios to compare VAE incidence between subjects with known and unknown PFO status, was not possible. Instead, weighted summary rates and a 95% confidence interval (CI) of VAE incidence was produced, using the random effects metaanalysis model for known and unknown PFO status. Using this methodology, each study was weighted fairly, with more weight given to studies with larger sample sizes, especially when the interstudy variation was larger than the intrastudy variation for VAE incidence. After weighting, subject outcomes for the known and unknown PFO status populations were compared using a z-test with the estimated proportions and variances. The systematic-analysis was performed using the Comprehensive Meta-Analysis software package (Biostat Inc., Englewood, NJ, USA).
Results
There were 40 studies published between 1972 and April 2014 that met the inclusion-exclusion criteria; 27 for group 1 (Table1) and 13 for group II (Table 2). Among these articles, 38 were in English, and 2 were in French, with all abstracts available in English. A total of 8,890 subjects were included, with 6,495 subjects in group I and 2,395 in group II. The sample size ranged between 15 and 799 subjects. Subjects’ age ranged between 6 weeks and 82 years. The study sites were located in the US, Germany, France, the UK, Japan, Turkey and Finland, among several other countries. Of all included studies, 17 were prospective, 21 retrospective, and 2 combined retrospective and prospective methods.
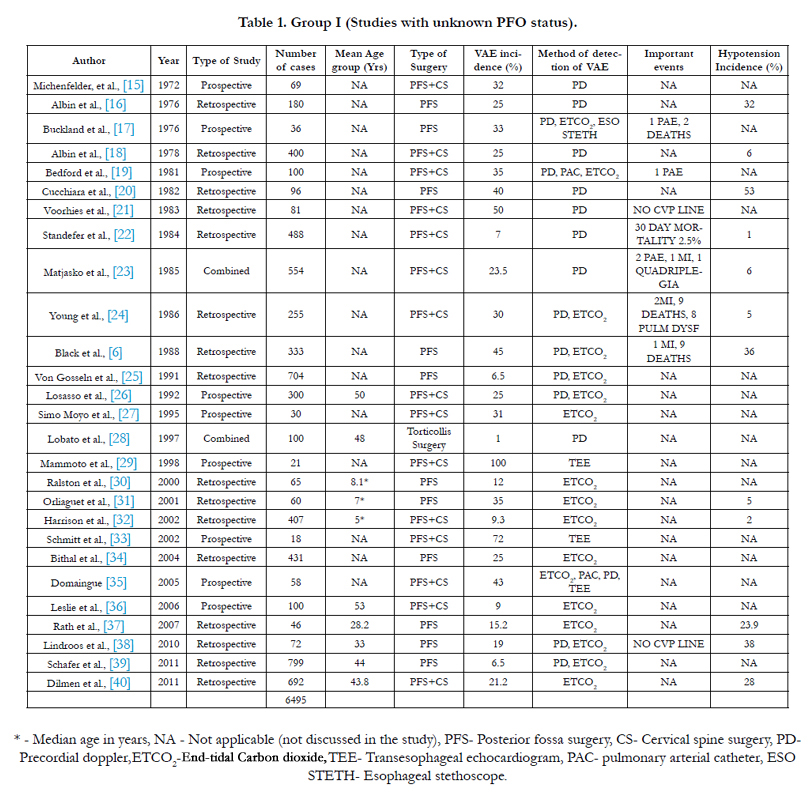

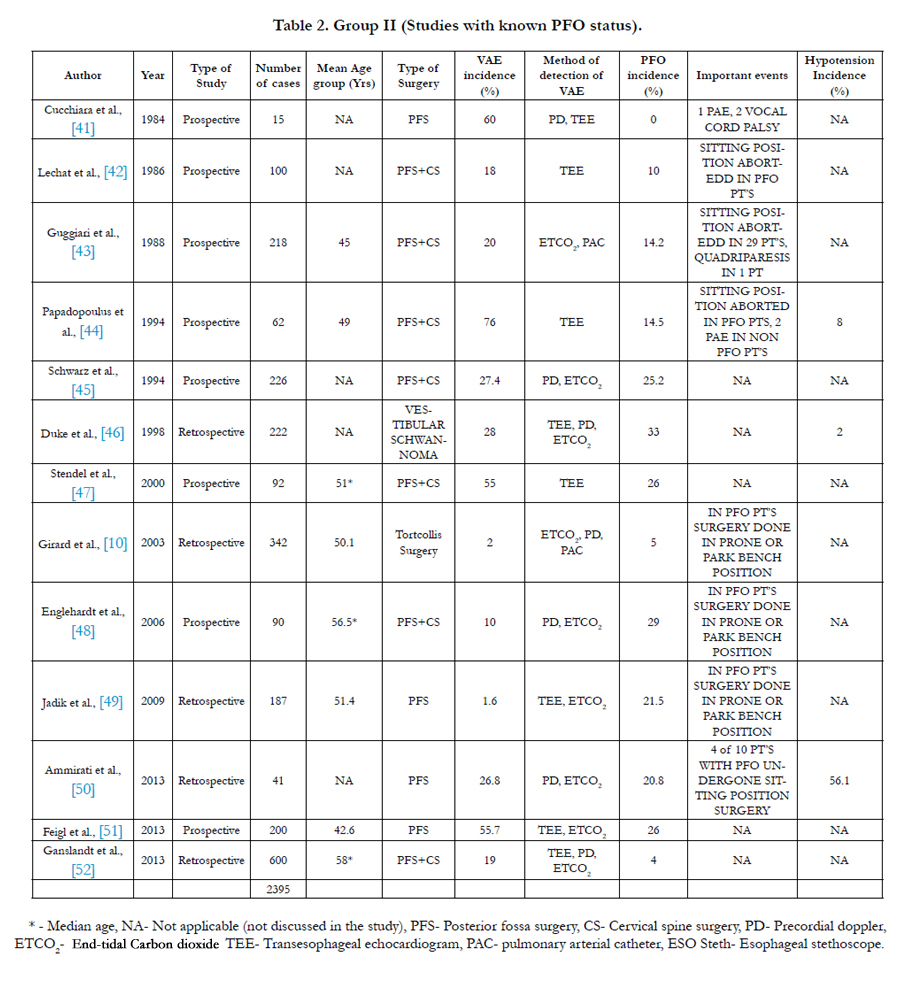
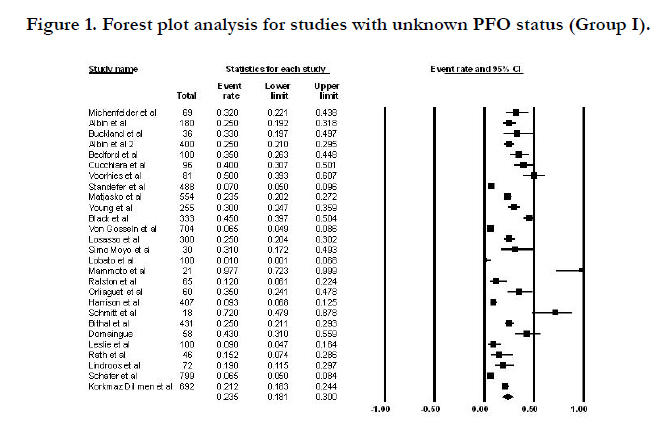
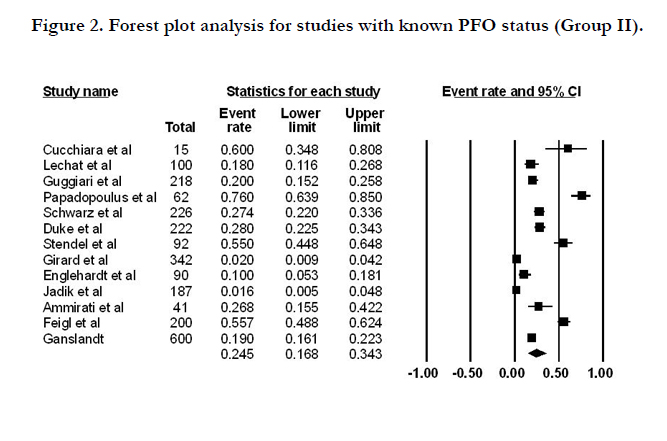
Using a random-effect model, the estimated VAE incidence rate for unknown PFO status was 23.5% with a 95% confidence interval (CI) of 18.1‒30%; the estimated VAE incidence rate for known PFO status was 24.5%, with a 95% CI of 16.8‒34.3%. Even within group II, the incidence and complication rates for subjects with known PFO status, who underwent neurosurgical procedures in the SSP, were comparable with those obtained for subjects who had not undergone semisitting neurosurgical procedures. The VAE incidence rate did not differ significantly between the two groups, (p = 0.88; z-test). The forest plots displayed in (Figures 1‒2) illustrate the VAE incidence rate with 95% CIs for each individual study, and the overall VAE incidence rate. Other complications, including PAE, hypotension, MI, stroke and perioperative deaths, could not be compared between the two groups due to inadequate power.
Discussion
In 1931, Dr. Thierry de Martel introduced the SP for patients undergoing neurosurgical procedures[1]. Subsequently, the SSP replaced the SP, including its associated risks. The SSP confers both benefits and risks for PFS and CSS. Current indications for semisitting craniotomy include PFS, tumors, AVMs, aneurysms, CSS, and subtemporal approaches to the intracranial fossa. Absolute contraindications include a functioning ventriculo-atrial shunt, right atrial pressure in excess of left atrial pressure with an intracardiac shunt, and cerebral ischemia when the patient is upright and awake. Relative contraindications include extremes of age, uncontrolled hypertension, and COPD [13]. Jadik et alproposed the semisitting position, it is the modification of initial sitting position, aiming to achieve a positive venous pressure at the operation site and increase the safety of the procedure [49]. The positioning requires a combination of adjustments of upper body and legs elevated by bending the operating table to a position where the hip is flexed to a maximum of 90 degrees. A 30 degrees flexion of the knees is maintained to avoid overstretching of the tendons and nerves of the leg. The patient's head is flexed anteriorly and a 2-finger space between the sternal notch and the chin to avoid cerebral venous outflow obstruction. Arms are supported to avoid traction of the shoulders; legs, arms and heels are padded. Finally, the inclination of the whole operating table is changed to lower the head and higher legs position, where the legs of the patients are as high as the vertex. This modified position has been included in quite all recent prospective published series from different countries. Advantages of the SSP for craniotomy include improved surgical exposure for midline lesions in the posterior cranial fossa, superior anatomical orientation with less injury to vital structures, reduced cranial nerve manipulation, improved venous drainage with superior hemostasis, gravitational drainage of CSF with decreased ICP, improved access to the patient’s face and chest, improved respiratory dynamics, and a shorter surgical time. Complications include VAE, systemic hypotension, postoperative tension pneumocephalus, subdural hematoma, quadriplegia, cranial nerve damage, macroglossia and peripheral nerve damage. Multiple studies within the case series linked the presence of an intracardiac shunt (PFO) with instances of VAE and PAE in patients undergoing craniotomies in the SSP. Such studies prompted disuse of the position in Western countries [6,8,11,12].
Management of VAE in the SSP starts with thorough evaluation and preparation of the patient during the preoperative period and good communication between the team members in the operating room, including the neurosurgeon and anesthesiologist. With the first identification or suspicion of VAE during surgery, the anesthesiologist should notify the surgeon to reduce further air entrainment and VAE size from the surgical field by flooding the surgical site with saline, placing the bone wax over bony edges to prevent air entrainment through open venous system of skull, 100% oxygen administration, lowering the head (if possible), increasing venous pressure using bilateral jugular venous compression, administering intravenous fluids, and by aspiration of air through the central venous catheter [22,23].
Seward et al. (1975) first described the clinical use of intravenously administered aerated saline, as a contrast during M-mode contrast echocardiographyp[57,58] With subsequent advances in this technology, transesophageal echocardiography (TEE) was introduced to diagnose air embolisms in neurosurgical patients. TEE was found to be more sensitive than PD, PA and CVP catheters, end-tidal CO2 and esophageal stethoscopes, for the detection of VAE at volumes of 0.01 mL/kg. Comparative studies of PFO and VAE detection methods conclude that TEE is the gold standard for detection, both preoperatively and intraoperatively [47,59]. However, TEE also has complications, of which the most-important are acute trauma to pharyngeal structures and esophagus and vocal cord paralysis[41,57].
Current preoperative practice for elective semisitting craniotomy includes evaluation for intracardiac shunt (PFO) by TEE, TTE or TCD. TEE is performed by the cardiologist as an ambulatory evaluation, or in the operating room after induction of anesthesia. Intracardiac shunt and flow directions were better-identified by a saline contrast agitation test in TEE; its sensitivity, and PFO identification rate (26%), is higher compared to TTE (10.8%) and TCD (23.9%) [10,11,13,56,59,60]. Even following the exclusion of PFO by preoperative TEE, intrapulmonary functional arteriovenous anastomoses may still lead to extra-cardiac PAE in certain patients undergoing semisitting neurosurgical procedures [61]. In a prospective study by Papadopoulos et al. (1994), two patients experienced PAE despite preoperative TEE screening [44]. In cases of both PAE and PFO during semisitting neurosurgical procedures, venous injury at the surgical site with air entrainment rather than the intracardiac shunt itself is of primary concern. To date, no official guidelines have been formulated regarding when a PFO should be considered an absolute contraindication for surgery, and when the intervention should proceed.
Thus far, prospective and retrospective studies have drawn their conclusions based on personal experiences and the grading systems developed to assess VAE [7,10,25,28,49,51,62,63]. In a study conducted by Fathi et al., patients with PFO underwent interventional closure 2‒4 weeks before their neurosurgical procedure in the SSP [5] Although PFO closure is performed as an ambulatory procedure, it exposes the patient to the risks of a second procedure, and increases the economic burden on healthcare systems. Even after PFO closure, a residual shunt may still present, although this shunt does not confer a sizable risk for neurological patients.64 Technical problems associated with PFO closure include the fact it is feasible only during elective neurosurgery, and the risk of closure failure in certain patients. In such cases, the neurosurgical procedure is performed in the horizontal position [5]
The VAE incidence rate for patients undergoing neurosurgery in the SSP has been reported at 39% for PFS and 11% for CSS. The majority of studies demonstrate a low incidence of PAE, ranging between 0‒14%. However, in all reported cases, the identification of PAE was achieved only after surgery utilizing non-standard, inaccurate methods of detection and incomplete data registration [5,17,29,41,44]. Ischemic brain injury and other types of organ damage have been identified as possible sequelae of PAE after SP neurosurgical procedures [5,57,65-71]. Prior to 2013, such risks rendered PFO contraindicatory for neurosurgery in the SSP, with the prone or park bench positions used instead. More recently, studies by Ammirati et al. (4 patients), Feigl et al. (52 patients) and Genslandt et al. (24 patients) have altered this clinical practice and reported VAE prevalence rates of 26.8%, 55.7%, and 19%, respectively, in patients with diagnosed PFOs. Moreover, these rates did not differ significantly between surgical populations with and without a PFO [50,51,52].
Our systematic analysis obtained similar results. The incidence of VAE did not differ significantly between groups with unknown and known PFO status (23.5% and 24.5%, p = 0.88). Comparison of other complications, including PAE, hypotension, myocardial infarction, stroke and death, were not feasible due to variation in data reportage among studies. As suggested by Kaye et al., the most-robust experimental model would include patients presenting with PFS or CSS, randomized to the SSP or a non-SSP after standardization of anesthesia and surgical techniques [72]. “However, no audit will resolve the issues of the selection of suitable patients and their intra- and post-operative management” [73-74].
Until further literature is available providing definitive guidelines, it is prudent to adhere to the basic physiologic concepts of SSP management and employ advanced monitoring techniques, such as TEE preoperatively to evaluate the size and flow direction of intracardiac shunts, and use intraoperative standard ASA monitors with arterial line and central venous catheters, with proper positioning at the junction of the superior vena cava and right atrium, and precordial Doppler to optimize clinical practice during the management of neurosurgical procedures conducted in the SSP for PFO patients. Each planned neurosurgical procedure that involves the SSP should be evaluated in terms of risks and benefits to provide superior patient outcomes.
Study Limitations
The results of the current study, with respect to its clinical relevance, must be interpreted with caution. In terms of limitations, the first and most important caveat is the potential bias introduced by the design of the studies included in the systematic analysis, because they were non-randomized and not adjusted for non-confounding variables. The second limitation concerns variation in the sample size of each group (lack of level A evidence). Third, in the majority of the observational and retrospective studies included,the methods used for case allocation and patient selection were not clear. Fourth, in group 1 (patients with unknown PFO) the patient was not certain to be free of PFO, considering that the prevalence of PFO is approximately 25% (10‒35%). Fifth, there are currently no specific guidelines pertaining to neurosurgical procedures performed in the SSP, nor to monitoring, such that we must depend on the opinions professed in the studies reviewed herein.
Conclusions
In summary, the results of our systematic-analysis clearly show that there is no difference among patients in VAE incidence, provided a standardized approach is applied with respect to patient selection and monitoring methods during semisitting neurosurgical procedures. Neurosurgical procedures in the SSP can be performed safely under conditions of precise assessment of inherent, potential, and unavoidable risks. Patient positioning should be determined not only on the basis of intracardiac shunt, but should also take into consideration all of the potential benefits and risks of a particular position, and its effects on the overall outcome. Furthermore, stricter guidelines should be developed based on properly designed, multicenter prospective studies to clarify the indications and risks of the SSP during neurosurgery.
References
- De Martel T (1931) Surgical treatment of cerebral tumors. Technical considerations. Surg GynecolObstet.52:381-385
- Barlow J. An account of the removal of a tumor situated on the cheek. Roc- MedChirSoc 1830; 16: 19
- Hagen PT, Scholz DG, Edwards WD (1984) Incidence and size of patent foramen ovale during the first 10 decades of life. an autopsy study of 965 normal hearts. Mayo Clin Proc. 59(1): 17–20.
- Lechat P, Mas JL, Lascault G, Loron P, Theard M et al., (1988) Prevalence of patent foramen ovale in patients with stroke. N Engl J Med. 318 (18):1148– 52.
- Fathi AR, Eshtehardi P, Meier B( 2009) Patent foramen ovale and neurosurgery in sitting position: a systematic review. Br J Anaesth.102(5):588-96.
- Black S, Ockert DB, Oliver WC Jr, Cucchiara RF (1988) Outcome following posterior fossa craniectomy in patients in the sitting or horizontal positions. Anesthesiology. 69(1) 49–56.
- Domaingue CM (2005) Anaesthesia for neurosurgery in the sitting position: a practical approach. Anaesth Intensive Care. 33(3): 323–31.
- Elton RJ, Howell RS ( 1994) The sitting position in neurosurgical anaesthesia. a survey of British practice in 1991. Br J Anaesth. 73(2): 247– 248.
- Gale T, Leslie K (2004) Anaesthesia for neurosurgery in the sitting position. J ClinNeurosci. 11(7): 693–6.
- Girard F, Ruel M, McKenty S, Boudreault D, Chouinard P, et al., (2003) Incidences of venous air embolism and patent foramen ovale among patients undergoing selective peripheral denervation in the sitting position. Neuro-surgery.53: 316–9discussion 319–20.
- Leonard IE, Cunningham AJ (2002) The sitting position in neurosurgerynot yet obsolete. Br J Anaesth. 88(1): 1–3.
- Liutkus D, Gouraud JP, Blanloeil Y (2003) The sitting position in neurosurgical anaesthesia. a survey of French practice. Ann Fr Anesth Reanim. 22(4) 296–300.
- Porter JM, Pidgeon C, Cunningham AJ (1999) The sitting position in neurosurgery: a critical appraisal. Br J Anaesth. 82(1): 117–28.
- Schaffranietz L, Gunther L (1997) The sitting position in neurosurgical operations. Results of a survey. Anaesthesist. 46(2): 91–5.
- Michenfelder JD, Miller RH, Gronert GA (1972) Evaluation of an ultrasonic device (Doppler) for the diagnosis of venous air embolism. Anesthesiology.36(2) 164–7.
- Albin MS, Babinski M, Maroon JC (1976) Anesthetic management of posterior fossa surgery in the sitting position. ActaAnaesthesiolScand. 20(2) 117–128.
- Buckland RW, Manners JM (1976) Venous air embolism during neurosurgery. A comparison of various methods of detection in man. Anaesthesia 31(5) 633–43.
- Albin MS, Carroll RG, Maroon JC (1978) Clinical considerations concerning detection of venous air embolism. Neurosurgery 3(3) 380-4.
- Bedford RF, Marshall WK, Butler A, Welsh JE (1981) Cardiac catheters for diagnosis and treatment of venous air embolism: a prospective study in man. J Neurosurg. 55(4):610-4.
- Cucchiara RF, Bowers B (1982) Air embolism in children undergoing suboccipital craniotomy. Anesthesiology. 52(4):338-339.
- Voorhies RM, Fraser RA, Van Poznak A (1983) Prevention of air embolism with positive end expiratory pressure. Neurosurgery 12: 503–506.
- Standefer M, Bay JW, Trusso R (1984) The sitting position in neurosurgery. a retrospective analysis of 488 cases. Neurosurgery. 14(6): 649–58.
- Matjasko J, Petrozza P, Cohen M, Steinberg P (1985) Anesthesia and surgery in the seated position: analysis of 554 cases. Neurosurgery. 17(5): 695–702.
- Young ML, Smith DS, Murtagh F (1986) Comparison of surgical and anesthetic complications in neurosurgical patients experiencing venous air embolism in the sitting position. Neurosurgery 18(2) :157–61.
- vonGösseln, HH, Samii M, Suhr D (1991) The lounging position for posterior fossa surgery: anesthesiological considerations regarding air embolism. Childs Nerv Syst. 7(7):368-374.
- Losasso TJ, Muzzi DA, Dietz NM (1992) Fifty percent nitrous oxide does not increase the risk of venous air embolism in neurosurgical patients operated upon in the sitting position. Anesthesiology. 77(1): 21–30.
- Simo Moyo J, Adnet P, Wambo M (1995) Detection of gas embolism in neurosurgery by capnography. Apropos of 32 patients surgically treated in seated position. CahAnesthesiol.43(1): 77-9.
- Lobato EB, Black S, De Soto H (1997) Venous air embolism and selective denervation for torticollis. AnesthAnalg. 84(3):551-3.
- Mammoto T, Hayashi Y, Ohnishi Y (1998) Incidence of venous and paradoxical air embolism in neurosurgical patients in the sitting position: detection by transesophageal echocardiography. ActaAnaesthesiolScand 42 (6):643–7.
- Ralston C, Tatman A (2000) An audit of serious complications during neurosurgery in children using the sitting position. PaediatrAnaesth. 10(6): 698-9.
- Orliaguet GA, Hanafi M, Meyer PG, Blanot S, Jarreau MM, et al., (2001) Is the sitting or the prone position best for surgery for posterior fossa tumors in children? PaediatrAnaesth.11(5): 541-7.
- Harrison EA, Mackersie A, McEwan A, Facer E (2002) The sitting position for neurosurgery in children.a review of 16 years’ experience. Br J Anaesth 88(1): 12–7.
- Schmitt HJ, Hemmerling TM (2002) Venous air emboli occur during release of positive end-expiratory pressure and repositioning after sitting position surgery. AnesthAnalg . 94(2): 400–3 table of contents.
- Bithal PK, Pandia MP, Dash HH (2004) Comparative incidence of venous air embolism and associated hypotension in adults and children operated for neurosurgery in the sitting position. Eur J Anaesthesiol. 21(7): 517–22.
- Domaingue CM (2005) Neurosurgery in the sitting position: a case series. Anaesth Intensive Care.33(3): 332–5.
- Leslie K, Hui R, Kaye AH (2006) Venous air embolism and the sitting position:a case series. J ClinNeurosci. 13(4): 419–22.
- Rath GP, Bithal PK, Chaturvedi A, Dash HH (2007) Complications related to positioning in posterior fossa craniectomy. J ClinNeurosci. 14(6): 520–5.
- Lindroos AC, Niiya T, Randell T, Romani R, Hernesniemi J ,et al., (2010) Sitting position for removal of pineal region lesions: the Helsinki experience.World Neurosurg. 74(4-5):505-13.
- Schäfer ST, Sandalcioglu IE, Stegen B, Neumann A, Asgari S , et al., (2011) Venous air embolism during semi-sitting craniotomy evokes thrombocytopenia. Anaesthesia. 66(1):25-30.
- Dilmen OK, Akcil EF, Tureci E, Tunali Y, Bahar M, et al., (2011) Neurosurgery in the sitting position: retrospective analysis of 692 adult and pediatric cases. Turk Neurosurg. 21(4):634-40.
- Cucchiara RF, Nugent M, Seward JB, Messick JM (1984) Air embolism in upright neurosurgical patients: detection and localization by two-dimensional transesophageal echocardiography. Anesthesiology. 60(4): 353–5.
- Lechat P, Guggiari M, Lascault G, Fuschiardi M, Evans J, et al. (1986) Detection by contrast ultrasonography of patent foramen ovale before neurosurgery. Presse Med 15(30): 1409–10.
- Guggiari M, Lechat P, Garen-Colonne C, Fusciardi J, Viars P (1988) Early detection of patent foramen ovale by two-dimensional contrast echocardiography for prevention of paradoxical air embolism during sitting position. AnesthAnalg. 67(2):192-4.
- Papadopoulos G, Kuhly P, Brock M, Rudolph KH, Link J, et al., (1994) Venous and paradoxical air embolism in the sitting position. A prospective study with transoesophageal echocardiography. ActaNeurochir (Wien). 126 (2-4): 140–3.
- Schwarz G, Fuchs G, Weihs W, Tritthart H, Schalk HV, et al.,(1994) Sitting position for neurosurgery: experience with preoperative contrast echocardiography in 301 patients. J NeurosurgAnesthesiol. 6(2): 83–8.
- Duke DA, Lynch JJ, Harner SG, Faust RJ, Ebersold MJ (1998) Venous air embolism in sitting and supine patients undergoing vestibular schwannoma resection. Neurosurgery. 42(6) : 1282–6.
- Stendel R, Gramm HJ, Schröder K, Lober C, Brock M. (2000) Transcranial Doppler ultrasonography as a screening technique for detection of a patent foramen ovale before surgery in the sitting position. Anesthesiology. 93:971–5.
- Engelhardt M, Folkers W, Brenke C, Scholz M, Harders A,et al., (2006) Neurosurgical operations with the patient in sitting position: analysis of risk factors using transcranial Doppler sonography. Br J Anaesth.96(4): 467–72.
- Jadik S, Wissing H, Friedrich K, Beck J, Seifert V, et al.,(2009) A standardized protocol for the prevention of clinically relevant venous air embolism during neurosurgical interventions in the semisitting position. Neurosurgery.64(3): 533-8.
- Ammirati M, Lamki TT, Shaw AB, Forde B, Nakano I, et al., (2013) A streamlined protocol for the use of the semi-sitting position in neurosurgery: a report on 48 consecutive procedures. J ClinNeurosci. 20(1):32-4.
- Feigl GC, Decker K, Wurms M, Krischek B, Ritz R, et al.,(2014) Neurosurgical Procedures in the Semisitting Position: Evaluation of the Risk of Paradoxical Venous Air Embolism in Patients with a Patent Foramen Ovale. World Neurosurg. 81(1):159-64.
- Ganslandt O, Merkel A, Schmitt H, Tzabazis A, Buchfelder M, et al., (2013) The sitting position in neurosurgery: indications, complications and results. a single institution experience of 600 cases. ActaNeurochir (Wien).155(10):1887-93.
- Stroup DF, Berlin JA, Morton SC, et al., (2000) Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA. 283(15): 2008–2012.
- Moher D, Liberati A, Tetzlaff J, et al., (2009) PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J ClinEpidemiol. 62: 1006–1012.
- Siwek J, Gourlay ML, Slawson DC, et al., (2002) How to write an evidencebased clinical review article. Am Fam Physician. 65(2): 251–8.
- Schaffranietz L, Grothe A, Olthoff D (2000) Use of the sitting position in neurosurgery. Results of a 1998 survey in Germany. Anaesthesist.; 49(4): 269–74.
- Furuya H, Suzuki T, Okumura F, Kishi Y, Uefuji T (1983) Detection of air embolism by transesophageal echocardiography. Anesthesiology. 58(2): 124–9.
- Contrast Echocardiography. Developments in Cardiovascular Medicine Series, Volume:15 Edited by Meltzer RF, Roelandt J. Springer, The Hague/ Boston/London, MartnusNighoff Publishers 1982.
- Mirski MA, Lele AV, Fitzsimmons L, Toung TJ (2007) Diagnosis and treatment of vascular air embolism. Anesthesiology. 106(1): 164-77.
- Kwapisz MM, Deinsberger W, Müller M, Nopens H, Neuhäuser C, et al., (2004) Transesophageal echocardiography as a guide for patient positioning before neurosurgical procedures in semi-sitting position. J Neurosurg Anesthesiol;16(4): 277–81.
- Schlundt J, Tzanova I, Werner C (2012) A case of intrapulmonary transmission of air while transitioning a patient from a sitting to a supine position after venous air embolism during a craniotomy. Can J Anaesth. 59(5): 478-82.
- Buis DR, Lai YM (2014) Use of Grading Scales in Venous Air Emboli During Neurosurgery. World Neurosurg. 81(6): e31.
- Misra BK (2014) Neurosurgery in the Semisitting Position in Patients with a Patent Foramen Ovale. World Neurosurg. 82(1): e41-2.
- Braun MU, Fassbender D, Schoen SP, Haass M, Schraeder R, et al., (2002) Transcatheter closure of patent foramen ovale in patients with cerebral ischemia. J Am CollCardiol. 39(12): 2019–25.
- Cucchiara RF, Seward JB, Nishimura RA, Nugent M, Faust RJ (1985) Identification of patent foramen ovale during sitting position craniotomy by transesophageal echocardiography with positive airway pressure. Anesthesiology.63(1): 107–9.
- Garachemani A, Eshtehardi P, Meier B (2007) Paradoxical emboli through the patent foramen ovale as the suspected cause of myocardial and renal infarction in a 48-year-old woman. Catheter CardiovascInterv; 70(2): 1010–2.
- Gronert GA, Messick JM Jr, Cucchiara RF, Michenfelder JD (1979) Paradoxical air embolism from a patent foramen ovale. Anesthesiology. 50(6):548–9.
- Loscalzo J (1986) Paradoxical embolism: clinical presentation, diagnostic strategies, and therapeutic options. Am Heart J. 112(1): 141–5.
- Perkins-Pearson NA, Marshall WK, Bedford RF (1982) Atrial pressures in the seated position: implication for paradoxical air embolism. Anesthesiology.57(6): 493–7.
- Thompson T, Evans W. Paradoxical embolism. Q J Med 1930;23: 135–50.
- Windecker S, Wahl A, Chatterjee T, Garachemani A, Eberli FR, et al.,(2000) Percutaneous closure of patent foramen ovale in patients with paradoxical embolism: long-term risk of recurrent thromboembolic events. Circulation.101(8): 893–8.
- Kaye AH, Leslie K (2012) The sitting position for neurosurgery: yet another case series confirming safety. World Neurosurg. 77(1): 42-3.
- Leslie K, Kaye AH (2013) The sitting position and the patent foramen ovale. Commentary: "A streamlined protocol for the use of the semi-sitting position in neurosurgery". J ClinNeurosci. 20(1): 35-6.
- Nozaki K (2014) Selection of Semisitting Position in Neurosurgery: Essential or Preference?. World Neurosurg. 81(1): 62-3.





