Spinal Anesthesia as an Alternative to General Anesthesia for Emergency Laprotomies in ASA Grade III And IV Patients. an Observational Study
Chavan G1*, Aparna Chavan2
1 Jawaharlal Nehru Medical College, India.
2 Department of ENT, JNMC, Associate Professor Sawangi Meghe, Wardha, India.
*Corresponding Author
Gajanan Chavan,
Jawaharlal Nehru Medical College,
India.
E-mail: gcgcny@gmail.com
Received: March 04, 2016; Accepted: May 03, 2016; Published: May 04, 2016
Citation: Chavan G (2016) Spinal Anesthesia as an Alternative to General Anesthesia for Emergency Laprotomiesin ASA Grade III And IV Patients. an Observational Study. Int J Anesth Res. 4(5), 236-238.DOI : dx.doi.org/10.19070/2332-2780-1600053
Copyright: Chavan G© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Prevalence of smoking and excessive consumption of alcohol is very high in rural parts of Telangana. The common complications due to this habit may lead to development of COPD in smokers , as well as development of gastro duodenal ulcers. Perforation peritonitis is also very rampant in this part of India. It is well known that smokers and patients with COPD have higher rate of pulmonary related complications following abdominal surgery.
Non availability of modern ventilatory facilities at these areas is still a major concern as well as challenge to the practicing anesthesiologist in these parts of India. Delayed diagnosis and late referral of abdominal emergencies to the referral centers makes it more difficult to manage and provide optimal care, however due to poor financial status and critical conditions it is never easy to refer them to tertiary centers with these facilities. This study review the utility of spinal anesthesia in such cases.
Material and Methods: We reviewed all cases of abdominal laprotomies conducted during period of June 2008- May 2010. Total 56 cases were selected who were given spinal anesthesia as a sole anesthetic and were chronic smokers with evidence of COPD. 25cases were of ASA grade IV and 31were grade III. All cases were operated for perforation peritonitis. Outcome of these cases was recorded and analyzed.
Results: Intraoperative conditions were adequate with spinal anesthesia alone for successful completion of the procedure in all cases except 2(1.12%)cases needed GA due to prolong surgical time. None needed mechanical ventilation in postoperative period , 2 patients have developed pneumonia, and mean length of hospital stay was 7 days. There was no report of renal or respiratory insufficiency.
Conclusion: Emergency laprotomies can be safely performed under Spinal anesthesia, making it a safe option and alternative to GA at the centers without modern ventilatory care.
2.Introduction
3.Material & Method
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
ASA; Spinal Anesthesia; Emergency Laprotomies; Smokers; COPD; Postoperative Outcome
Introduction
Compared to the normal population postoperative complications are 9.5 time more frequent in patients with pre-existing pulmonary diseases [1]. In particular, patients with chronic obstructive pulmonary disease (COPD) have a very high mortality risk of 5-13 times [2]. Postoperative pulmonary complications are highest among patients who undergo upper abdominal procedures [3]. Due to no availability of modern ventilatory care and ICU care mortality rate was very high in immediate postoperative period. Such high mortality may be due to the effects of general anesthesia (GA) and improper mechanical ventilation of the already compromised lungs, as well as, excessive use of long acting opiods for sever pain control ,which may further affect pulmonary function and leads to ventilator dependence.
Regional anesthesia (RA) may be an attractive and safe alternative to general anesthesia since neuroaxial blockade has minimal respiratory effects even at higher level block [4]. Certain retrospective [5] and prospective [6, 7] observational studies in the non thoracic surgical shows that patients with severCOPD [5] as well as patients not selected for pulmonary pathology [6, 7] have better respiratory outcomes when neuroaxial blockade is given rather than GA. Publications over the use of regional anesthesia as a sole anesthetic for upper abdominal surgeries is little, however, prospective randomized studies have been conducted which evaluate the outcome of combined general and regional anesthesia [9, 10]. A large matanalysis [8] of prospective, randomizes studies showed significant benefit to neuroaxial blockade in a large surgical population, but the study grouped RA and combined RA/GA patients together. Studies of abdominal surgery patients comparing the combined approach with GA alone consistently have shown trends toward decreased rates of postoperative failure [9, 10], presumably due to the superior postoperative pain control provided by the regional technique.
Our study provide evidence that many upper abdominal surgical procedures thought to require GA may be safely and effectively performed using spinal anesthesia alone. It may be seen that the postoperative course of these patients is incredibly smooth, allowing hospital discharge within several days of procedure.
Material & Method
After institutes ethic committees approval records of surgical patients operated for perforation peritonitis from medical record section was reviewed.
Patients who meet following criteria were selected
1. Chronic smokers of 45 years and above age.
2. Evidence of COPD on X-ray chest.
56 patients were identified(all male) ,and their records were reviewed to determine patient age,diagnosis,indications of surgery,type of surgery performed, American society of Anesthesiology (ASA) classification, need of GA, need for mechanical ventilation, length of stay, and perioperative complications or mortality.
Data was collected and analysed.
Results
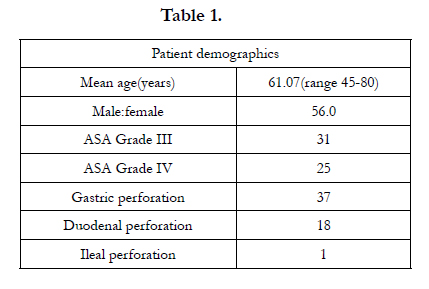
The average age of patients was 61.07years (Table 1). 37 patients were operated for gastric perforation, 18 patients for duodenal perforation and 1 was operated for ileac perforation. All the patients were assessed with American society of Anesthesiologist , 31 of them were ASA grade III ,and, 25 of them were classified as ASA grade IV.

All the patients were optimized preoperatively after initial assessment by Anesthesiologist(dehydration, electrolytes ,blood transfusion etc).
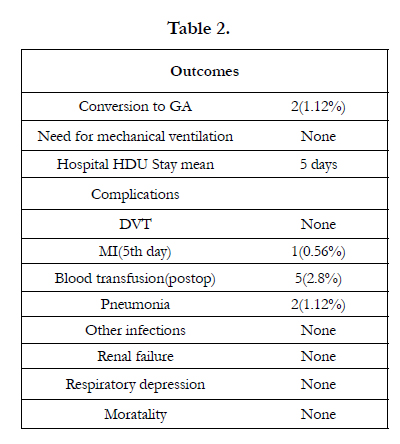
None patients had cardio respiratory arrest in perioperative period. Only 1.12%(2) patients needed GA due to prolong surgery, near end of surgery and that were successfully extubated on completion of the procedure. No patient.
needed mechanical ventilation in postoperative period. Mean length of stay in HDU(high dependency unit) was 5 days.
One (0.56%) patient have developed myocardial infraction on the 5th day of procedure and was treated with Streptokinase and was discharged after 15 day. 5(2.8%) patients were found to be anemic and received blood transfusion on 3rd postoperative day.
Two (1.12%) of the patients with history of recent respiratory tract infections have developed Pneumonia on 3rd day and were treated with higher antibiotics and discharged after 2 weeks. None of the patients have found to developed deep vein thrombosis, respiratory depression or renal failure. Overall mortality was zero. (Table 2).
Spinal block level attended was up to T4-T5 level, Intraoperative relaxation was adequate for successful completion of procedures.
Discussion
Although GA has the benefit of secured airway and to provide rest to respiratory muscles, however induction of GA and intubation of patients results in to dependence on mechanical ventilation. In addition to this there are mechanical as well as physiological effects of general anesthesia like bronchospasm, V/Q mismatch, atelectesis, effects on chest impedance, also ,use of large tidal volume or excessive PEEP may lead to pneumothorax in these patients and lastly there may be residual anesthetic or muscle relaxant effects. Considering these facts and taking account of the lack of modern ventilatory system at some institution, use of GA may increase risk of perioperative morbity and mortality.
Although subarachnoid block is not physiologically benign, it offers several advantages [8]. Upper abdominal surgery has detrimental effect on functional residual capacity. However, regional anesthesia attenuates this by improving diaphragmatic function and chest complaince,thus,normal minute volume is maintained. It also decreases lung congestion by decreasing preload and afterload.The benefits seen for neuroaxial blockade may be conferred by multifactorial mechanisms, including altered coagulation, improved ability to breath free of pain, and reduction in surgical stress response [11].
Overall mortality was reduced in patients allocated to neuroaxial blockade in a metanalysis done by Anthony Rodgers et al8,it also shows reduced odds of deep vein thrombosis, pulmonary embolism, blood transfusion requirement, pneumonia and respiratory depression. Our study also considered the same parameters and confirms same.
Conclusion
Although there is a need to conduct more prospective studies to best determine the clinical and surgical criteria for use of spinal anesthesia as a sole technique, our small observational study indicates the utility of spinal anesthesia in high risk ,smoker patients posted for upper abdominal surgery and more widespread use of this approach.
References
- Savas J, Litwack R (2004) Regional anesthesia as an alternative to general anesthesia for abdominal surgery in patients with severe pulmonary impairment. The American Journal of Surgery. 188(5): 603-605.
- Mallon J.S, Edelist G (1992) Risk factors of importance-the patient. Probl Anesth.6: 193-204.
- Brocks-Brunn, J.A (1997) Predictors of pulmonary complications following abdominal surgery. Chest. 111: 564-571.
- Askrog VF, Smith TC, Eckeenhoff JE (1964) Changes in pulmonary ventilation during spinal anesthesia. Surg Gynecol Obstet. 119: 563.
- Tarhan S, Moffit EA, Sessler AD (1973) Risk of anesthesia and surgery in patients with chronic bronchitis and obstructive pulmonary disease. Surgery.74(5): 720-6.
- Mitchell CK, Smoger SH, Pfiefer MP (1998) Multivariate analysis of factors associated with postoperative pulmonary complications folloeing elective surgery. Arch Surg. 133(2): 194-198.
- Arozullah AM, Khuri SF, Henderson WG, Daley J (2001) Development and validation of a multi factorial risk index for predicting postoperative pnumonia after major noncardiac surgery. Ann Intern Med. 135(10): 847-857.
- Anthony R. Walker N (2000) Reduction of postoperative mortality and morbidity with epidural or spinal anesthesia: results from overview of randomized trials. BMJ. 321(7275): 14993-1497.
- Woo YP, Thompson JS, Lee K.K (2001) Effect of epidural anesthesia and analgesia on perioperative and postoperative outcome: a randomized, controlled Veterans Affairs Cooperative study. Ann Surg. 234(4): 560-571.
- Rigg J.R, Jamrozik K (2002) Epidural anesthesia and analgesia and outcome of major surgery: a randomized trial. Lancet. 359((9314): 1276-1282.
- Kehlet H (1988) Modification of responses to surgical and neural blockade: Clinical implications. In: Neural Blockade in Clinical Anesthesia and Management of Pain, (2nd ed), Cousins MJ, Bridenbaugh PO (eds.). Philadelphia,JB Lippincott 145.





