Hemodynamic Influences of Angiotensin-Converting Enzyme Inhibitors on Patients Undergoing Total Knee Arthroplasty With Spinal Anesthesia
Pang H1*, Niebur P1, Karjalainen N1, Pellegrino K1, Christensen M1 , Lyden L2, Hoffman J1, Goergen K1
1 Department of Anesthesiology, University of Nebraska Medical Center, Omaha, NE 68198, USA.
2 Department of Biostatistics, College of Public Health, University of Nebraska Medical Center, Omaha, NE68198, USA.
*Corresponding Author
Huiling Pang MD. PhD,
Department of Anesthesiology
University of Nebraska Medical Center, Omaha, NE68198-4455, USA.
Tel. (402)559-4081
Fax (402)559-7372
E-mail: hpang@unmc.edu
Received: March 04, 2016; Accepted: April 11, 2016; Published: April 14, 2016
Citation: Pang H, et al. (2016) Hemodynamic Influences of Angiotensin-Converting Enzyme Inhibitors on Patients Undergoing Total Knee Arthroplasty With Spinal Anesthesia. Int J Anesth Res. 4(4), 219-224.DOI : dx.doi.org/10.19070/2332-2780-1600050
Copyright: Pang H© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Purpose: To determine if patients on angiotensin-converting enzyme inhibitors (ACEIs) had more severe hypotension or required higher doses of vasopressors compared to those who were not on ACEIs under spinal anesthesia for total knee arthroplasty (TKA).
Methods: A retrospective chart review of 169 patients who underwent TKA with spinal anesthesia between August 2012 and December 2014 was performed. The patients were divided into two groups, i.e. patients on ACEIs (ACEIs group) and patients not on ACEIs (non-ACEIs group), for comparison. The preoperative characteristics, anesthesia records, and postoperative outcomes were reviewed.
Results: The patients in the ACEIs group were more likely to have coexisting hypertension, diabetes mellitus, hyperlipidemia, and be on abeta blocker compared to patients in the nonACEIs group. All of the patients showed decreased blood pressure immediately post spinal injection. Patients in the ACEIs group had lower systolic blood pressure (SBP) and diastolic blood pressure (DBP)compared to the nonACEIs group at 10 minutes post spinal placement (p=0.01 for SBP and p= 0.005 for DBP). When comparing the two groups there was not a significant difference in severe hypotension or vasopressor requirements. However, the initial dose of propofol infusion for sedation was significantly lower in the ACEIs group (p=0.04)
Conclusion: Patients on ACEIs showed lower blood pressure shortly after spinal injection compared to patients not on ACEIs. However, the difference was small and transient. The requirements of vasopressors were not significantly higher in patients on ACEIs undergoing spinal anesthesia for TKA.
2.Introduction
3.Material & Method
3.1.Data collection
3.2.Statistical Analysis
4.Results
5.Discussion
6.Conclusion
7.Acknowledgements
8.References
Keywords
Angiotensin Converting Enzyme Inhibitors; Hypotension; Hemodynamic Changes; Spinal Anesthesia; Total Knee Arthroplasty.
Introduction
Total knee arthroplasty (TKA) is a surgical procedure performed for severe joint pain and osteoarthritis. There are approximately 700,000 TKAs performed in the United States every year with those numbers continuing to increase [1]. With the aging population, the number of patients undergoing TKA who have significant comorbidities is also increasing. Hypertension is the most common of these comorbidities with approximately 68% of TKA patients affected [2,3,4,5]. Controlling hypertension in the perioperative period is important to prevent serious complications including cardiovascular and renal events. Therefore, many patients are advised to continue taking their anti-hypertensive medicines up until and including the day of surgery.
While there are multiple classes of anti-hypertensive agents available, angiotensin converting enzyme inhibitors (ACEIs) are a class regularly used to treat patients with hypertension, especially in those with coexisting coronary artery disease, congestive heart failure, diabetes mellitus or kidney diseases [6]. ACEIs act to decrease the activity of the renin-angiotensin-aldosterone system by inhibiting the conversion of angiotensin I to angiotensin II, there by relaxing blood vessels, decreasing blood volume, and lowering blood pressure.
Regional anesthesia, mainly spinal anesthesia, has become the most popular anesthesia approach for TKA. Spinal anesthesia has been shown to decrease blood loss and the risk of thromboembolic events [7,8]. However, hypotension is common following spinal anesthesia because of the induced sympathetic block [9,10]. The concern remains that the combined hypotensive effects of spinal anesthesia and ACEIs may provoke significant hemodynamic instability resulting in adverse outcomes. The long-term clinical consequences of continuing versus withholding preoperative ACEIs are unknown [11,12,13,14]. Data from the literature investigating the effect of ACEIs on surgical patients under spinal anesthesia is limited. Currently, no consensus exists among anesthesiologists regarding whether one should continue ACEIs prior to TKA [4,13,15,16].
The aim of this retrospective study was to compare the hemodynamic effects observed in patients on ACEIs to those who were not on ACEIs in the setting of spinal anesthesia for TKA. Our focus was expanded to investigate if patients receiving ACEIs required higher doses of vasopressors compared to those who were not on ACEIs. Moreover, we were interested in identifying the differences in 30 day and 90 day readmission with regard to cardiac or pulmonary events between these two groups.
Material & Method
After obtaining Institutional Review Board approval of the University of Nebraska Medical Center, a retrospective chart review of all patients who underwent TKA between June 2012 and December 2014 was conducted. Of the 257 patients who had TKA during this time period, 88 patients received general anesthesia while 169 patients received spinal anesthesia. Patients who received general anesthesia or whose spinal anesthesia was not effective and converted to general anesthesia for the procedure were excluded. Only those 169 patients who received spinal anesthesia as their primary anesthetic technique for either a primary or revision of TKA were included in the final data analysis. According to the patient’s medication list at the time of surgery, the patients were divided into two groups for comparison, i.e. patients on ACEIs (ACEIs group) and patients not on ACEIs (nonACEIs group). The following data were collected with the RED Cap (Research Electronic Data Capture) tools: demographic characteristics, preoperative comorbidities, medication lists at the time of the procedure, anesthesia records during the time of surgery, post anesthesia care unit (PACU) records, postoperative reports until discharged from the hospital, and incidence of readmission within 30 and 90 days for adverse events including acute myocardial infarction, stroke, renal insufficiency, or pulmonary events. Systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR) prior to spinal injection, measurements taken every 5 minutes for up to 30 minutes post spinal placement, and upon PACU arrival were the focus of our comparison between the ACEI and nonACEI groups. The doses of propofol, phenylephrine, and ephedrine corresponding to these time periods were also compared.
Descriptive statistics (counts and percentages, means, standard deviations) were used to summarize the data. Fisher’s exact test was used to compare categorical data between the ACEIs and nonACEIs groups. Continuous variables were compared between the groups using the 2 sample t-testor Mann-Whitney test if the data was skewed. A comparison of the outcomes of SBP, DBP, and HR observed during surgery and in the PACU between the two groups was done using linear mixed effect models. The measurements of SBP, DBP and HR were considered as repeated measures in the models and fit with autoregressive (AR) (1) structure for correlations to evaluate the change in these measurements between any two measurement times while accounting for the within-subject correlation of repeated measures. Each outcome was evaluated separately and included a variable for group designation, time, and an interaction term for group and time. In addition, comparisons of the mean SBP, DBP and HR were done at each time point; p-values were unadjusted for these comparisons. SAS Version 9.4 was used for the analysis. All tests were 2-sided. A p-value < 0.05 was considered statistically significant.
Results
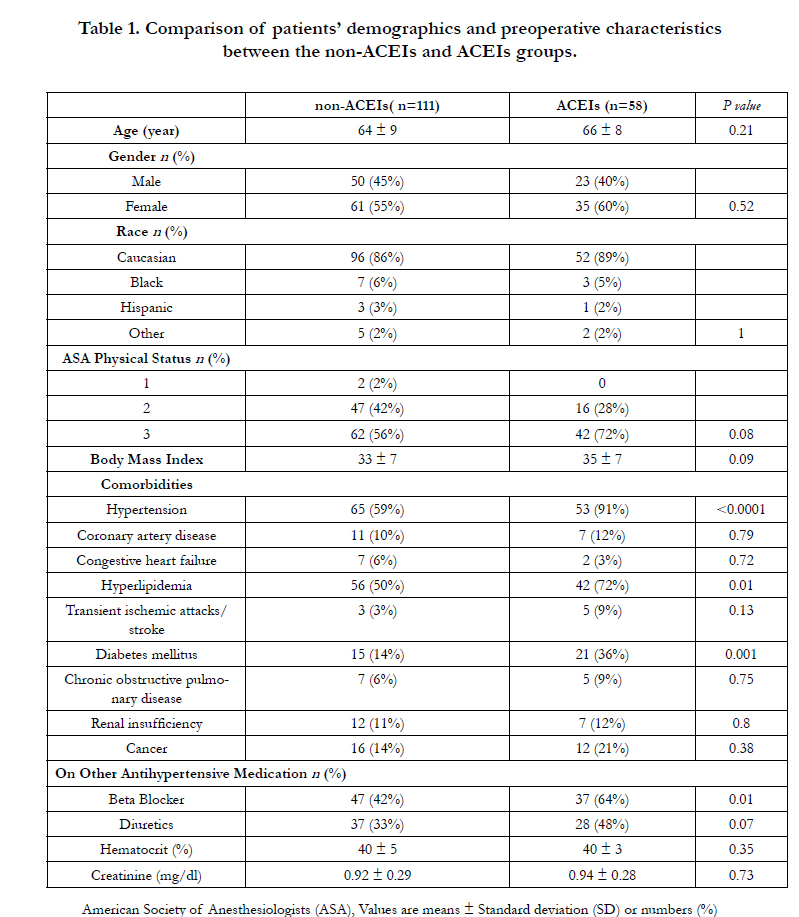
Among the total of 169 patients who received spinal anesthesia as their primary anesthetic technique for TKA, 58 patients were in the ACEIs group and 111 in the non ACEIs group. Demographic and preoperative characteristic data are shown in Table 1. Both groups were compatible regarding age, gender, race, American Society of Anesthesiologists (ASA) functional status, and body mass index (BMI). The majority of patients (72% in ACEIs group versus 56% in non ACEIs group) were functional class ASA 3. As expected, there were more patients with hypertension in the ACEIs group in comparison to the nonACEIs group (p<0.0001). There were also higher numbers of patients with diabetes mellitus (p= 0.001 ) and hyperlipidemia (p = 0.01) in the ACEIs group but no significant difference in other co-morbidities. Patients in the ACEIs group were more frequently on beta blockers (64% versus42%, p=0.01) and a trend toward significance ( p=0.07 is close to p<0.05 ) was found in terms of diuretics use between these two groups of patients.
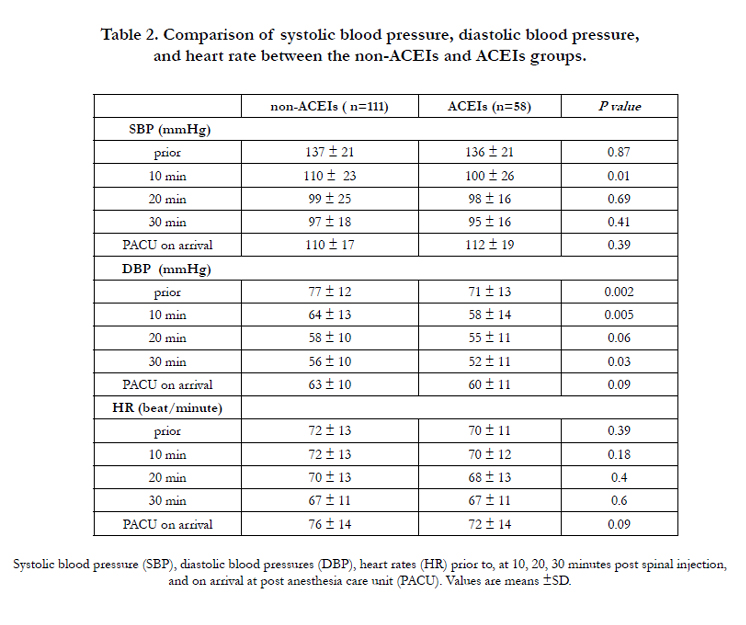
Comparisons of mean SBP, DBP, and HR prior to and at 10, 20, and 30 minutes post spinal anesthesia in patients in the non ACEIs versus the ACEIs groups are summarized in Table 2. Both groups showed decreased SBP and DBP immediately post spinal injection(Table 2).However, patients in the ACEIs group had lower mean DBPs throughout the time of surgery, includingthe starting DBP prior to spinal placement (p=0.002). Moreover, bothSBP and DBP were lower in patients in the ACEIs group versus the nonACEIs group at 10 minutes post spinal placement, which was statistically significant (p=0.01 for SBP and p= 0.005 for DBP). Except the results mentioned above, there were no significant differences of SBP, DBP, orHR observed during the times of surgery and on PACU arrival nor was there a significant interaction of time and ACEI grouping on the three outcomes during the surgery time period.
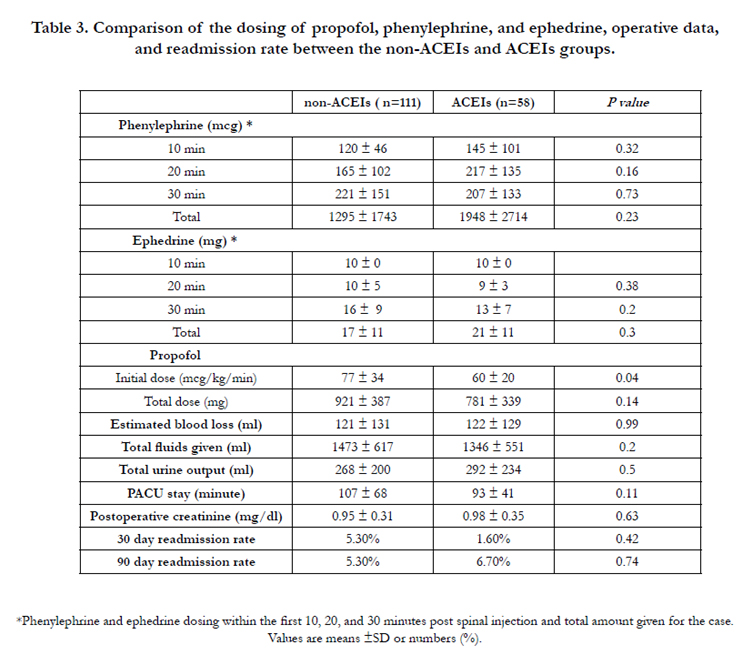
The observation of the hemodynamic changes between these two groups raises a question of whether vasoactive drugs such as phenylephrine or ephedrine were more aggressively given to the patients in ACEIs group, especially in the first 30 minutes post spinal placement. Our study did not find significant differences in phenylephrine or ephedrine administration between the two groups in the time frames of 10, 20, 30 minutes post spinal injection and the total amounts used (Table 3). However, although the total doses of propofol administered were not different between these two groups, the initial rate of propofol infusion was significantly lower (p=0.04) in the ACEIs group compared to the nonACEIs group (Table 3).There were no significant findings for estimate blood loss, total intravenous fluid use, urine output, postoperative creatinine level, and the length of PACU stay (Table 3). Our results did not reveal any observed difference in the rates of 30 day- and 90 day- readmissions between the ACEI and nonACEI groups.
Discussion
The aim of this retrospective study was to investigate perioperative hemodynamic influence of ACEIs on patients undergoing TKA. Our study showed that the comorbidities over-represented in the ACEIs group included hypertension, hyperlipidemia, and diabetes mellitus (Table 1). A logical explanation for this finding is that ACEIs and beta blockers are the commonly used medications for hypertension management in patients with these two metabolic syndromes [6,11,14]. Thesecomorbid conditions may have considerable impacts on perioperative outcome [2,3,4,5].

Maintaining mean blood pressure at 60-70 mmHg intraoperatively is generally preferred to minimize blood loss as well as to preserve adequate perfusion to vital organs, especially in patients with significant comorbidities. Our study revealed a lower mean DBP in the ACEIs group through out the time period during surgery (Table 2). The pharmacologic effects of ACEIs may be one of the factors associated with this finding [6,11,14].Notably, patients in the ACEIs group showed lower SBP and DBP at 10 minutes post spinal placement relative to patients in the nonACEIs group. This finding is consistent with the findings from previous studies in the literature that patients on ACEIs experienced an increased incidence of hypotensionpost spinal/epidural anesthesia [15,17,18]. However, even though our data indicated there were statistically significant differences of SBP and DBP between the ACEIsversus nonACEIs group, the clinical significance of these differences needs further assessment. It may seem reasonable to expect that patients in the ACEIs group would demand more aggressive treatment to attain optimal blood pressure. However, our study did not found such differences in terms of phenylephrine or ephedrine dosing. Instead, our data showed that the anesthesia providers were more likely to start propofol infusion at a lower rate for sedation in the ACEIs group post spinal injection. This measure may have compensated for the changes of blood pressure during the time period immediate post spinal placement. Similar findings reported in the literature stated that using decreased induction dose of propofol could easily reduce the need for hypotension correction in patients chronically taking ACEIs [19]. There was no data to draw conclusions regarding the effectiveness of other vaso active medications in the current study, since no records indicated epinephrine or vasopressin was given to these two groups of patients. Blood pressure and heart rate remained comparable in these two groups of patients later on in the procedure and on PACU arrival. No significant differences of the total dose of propofol administered were observed in these two groups. Therefore, although there was greater systolic and diastolic hypotension observed in the ACEIs group immediately post spinal placement, its clinical relevance may not be substantial. It is an interesting finding that the heart rates at all observed time points were not significantly different in these two groups of patients, even though higher numbers of patients in the ACEIs group were concurrently taking a beta blocker. The mechanisms in response to sympathetic block caused by spinal anesthesia may vary in these two groups of patients [12]. We recognized that the approach of the spinal anesthetics was not stringently standardized in these two groups of patients, which could potentially influence the clinical presentation. However, our patients typically received preservative-free hyperbaric bupivacaine (0.75% in dextrose, 1.8-2 mL) as the spinal agent and propofol infusion after spinal placement for intraoperative sedation. Spinal anesthesia received by these two groups of patients was likely very compatible and its impact on the hemodynamic differences observed between these two groups may be insignificant.
Data from the literature investigating the effect of ACEIs on surgical patients under regional anesthesia is very limited. Current literature remains equivocal regarding continuation of ACEIs preoperatively [6,11,13,14]. A previous studyreported that patients who received preoperative angiotensin axis blockadesundergoing major orthopedic surgeries, such as spinal fusion, hip or knee arthroplasty, have an associated increased risk of postinduction hypotension and postoperative acute kidney injury (AKI) resulting in a greater hospital length of stay [18]. Other studies have concluded that long term ACEIs treatment does not further exaggerate the blood pressure decrease in the early phase of spinal anesthesia and ACEIs are not associated with increased mortality after noncardiac surgery [16,20]. Our study did not reveal significant differences concerning postoperative change of serum creatinine level, the length of PACU stay, and 30 day- or 90 day-readmission rate. Further evidence is required to prove that preoperative ACEI therapy has a direct cause and effect relationship with serious perioperative complications including AKI. It is worth the consideration that postoperative rebound hypertension is a serious complication associated with adverted cardiovascular outcomes [21]. The American Heart Association/ American College of Cardiology (AHA/ACC) states that as a class I recommendation, ACEIs should be started and continued indefinitely in all patients with left ventricular ejection fraction less than 40% and in those with hypertension, diabetes, or chronic kidney disease, unless contraindicated. They further state, as a class IIb recommendation, that it is reasonable to use ACEIs in all other patients [22]. The result of our study is in agreement with the AHA/ACC recommendation to continue ACEIs perioperatively to prevent possible rebound hypertension and related serious sequelae. Further studies are required to demonstrate whether the organ-protective benefits of ACEIs validate their continuation in the perioperative setting.
We acknowledge there are several limitations in our study. This is a retrospective analysis over a selected period of time in a single academic medical center. Due to the retrospective observational nature of the study, the information obtained relies on prior medical records and the patients in the two study groups were not randomized. The type, dose, and duration of ACEIs taken by the patients were not specified. We did not further elucidate the possible influence of other blood pressure medications such as ARBs, calcium channel blockers, beta blockers, and diuretics on the results. Additionally, it is possible that boluses of vasopressors were not thoroughly documented by each individual provider. Although well-compatible with several relevant studies in the literature [9,10,15,19], the sample size of our study was still relatively small. Future prospective randomized studies with larger sample size may need to confirm our findings.
Conclusion
In conclusion, based on the current study, patients on ACEIs showed transient lower blood pressure shortly after spinal injection compared to patients not on ACEIs. The requirements of vasopressors were not significantly higher in patients on ACEIs undergoing spinal anesthesia for TKA.
Acknowledgements
We thank Austin M.Porter and Rachel Quandahl for assistance with data collection.
References
- Kurtz S, Ong K, Lau E, Mowat F, Halpern M (2007) Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am 89(4): 780-785.
- Memtsoudis SG, Della Valle AG, Besculides MC, Gaber L, Laskin R (2009) Trends in demographics, comorbidity profiles, in-hospital complications and mortality associated with primary knee arthroplasty. J Arthroplasty 24(4): 518-527.
- Oviedo Baena AM, Moeschler SM, Smith HM, Duncan CM, Schroeder DR, et al. (2015) Perioperative comorbidities and complications among patientsundergoing primary total knee arthroplasty: a retrospective analysis and prospective survey. J Clin Anesth 27(7): 558-565.
- Pugely AJ, Martin CT, Gao Y, Belatti DA, Callaghan JJ (2014) Comorbidities in patients undergoing total knee arthroplasty: do they influence hospital costs and length of stay? Clin Orthop Relat Res 472(12): 3943-3950.
- Zmistowski B, Dizdarevic I, Jacovides CL, Radcliff KE, Mraovic B, et al. (2013) Patients with uncontrolled components of metabolic syndrome have increased of complications following total joint arthroplasty. J Arthroplasty 28(6): 904-907.
- James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, et al. (2014) 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 311(5): 507-520.
- Pugely AJ, Martin CT, Gao Y, Mendoza-Lattes S, Callaghan JJ (2013) Differences in short-term complications between spinal and general anesthesia for primary total knee arthroplasty. J Bone Joint Surg Am 95(3): 193-199.
- Fleischut PM, Eskreis-Winkler JM, Gaber-Baylis LK, Giambrone GP, Faggiani SL, et al. (2015) Variability in anesthetic care for total knee arthroplasty: an analysis from the anesthesia quality institute. Am J Med Qual 30(2): 172-179.
- Meyhoff CS, Haarmark C, Kanters JK, Rasmussen LS (2009) Is it possible to predict hypotension during onset of spinal anesthesia in elderly patients? J Clin Anesth 21(1): 23-29.
- Nakasuji M, Suh SH, Nomura M, Nakamura M, Imanaka N, et al. (2012) Hypotension from spinal anesthesia in patients aged greater than 80 years is due to a decrease in systemic vascular resistance. J Clin Anesth 24(3):201-206.
- Comfere T, Sprung J, Kumar MM, Draper M, Wilson DP, et al. (2005) Angiotensin system inhibitors in a general surgical population. Anesth Analg 100(3): 636-644.
- Auron M, Harte B, Kumar A, Michota F (2011) Renin-angiotensin system antagonists in the perioperative setting: clinical consequences and recommendations for practice. Postgrad Med J 87(1029): 472-481.
- Bogebjerg MK (2012) No consensus on withholding angiotensin-converting enzyme inhibitors and angiotensin receptor blockers before spinal anaesthesia. Dan Med J 59(12): A4543.
- Mets B (2015) To stop or not? Anesth Analg 120(6): 1413-1419.
- Calloway JJ, Memtsoudis SG, Krauser DG, Ma Y, Russell LA, et al. (2014) Hemodynamic effects of angiotensin inhibitors in elderly hypertensives undergoing total knee arthroplaty under regional anesthesia. J Am Soc Hypertens 8(9): 644-651.
- Höhne C, Meier L, Boemke W, Kaczmarczyk G (2003) ACE inhibition does not exaggerate the blood pressure decrease in the early phase of spinal anaesthesia. Acta Anaesthesiol Scand 47(7): 891-896.
- Goodman SM, Krauser D, Mackenzie CR, Memtsoudis S (2012) Cardiac Arrest during Total Hip Arthroplasty in a Patient on an Angiotensin Receptor Antagonist. HSS J 8(2): 175-183.
- Nielson E, Hennrikus E, Lehman E, Mets B (2014) Angiotensin axis blockade, hypotension, and acute kidney injury in elective major orthopedic surgery. J Hosp Med 9(5): 283-288.
- Weisenberg M, Sessler DI, Tavdi M, Gleb M, Ezri T, et al. (2010) Dosedependent hemodynamic effects of propofol induction following brotizolam premedication in hypertensive patients taking angiotensin-converting enzyme inhibitors. J Clin Anesth 22(3): 190-195.
- Turan A, You J, Shiba A, Kurz A, Saager L, et al. (2012) Angiotensin converting enzyme inhibitors are not associated with respiratory complications or mortality after noncardiac surgery. Anesth Analg 114(3): 552-560.
- Twersky RS, Goel V, Narayan P, Weedon J (2014) The risk of hypertension after preoperative discontinuation of angiotensin-converting enzyme inhibitors or angiotensin receptor antagonists in ambulatory and same-day admission patients. Anesth Analg 118(5): 938-944.
- Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, et al. (2014) 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 64: e77-137.





