Day and Night Administration of Sevoflurane Effect of Melatonin Levels in Rats
Onay V1, Erdost HA1*, Ocmen E1, Akan P2, Gunenc F1, Arkan A1, Gokmen AN1
1 Anesthesiology, School of Medicine, Dokuz Eylul University, Izmir, Turkey.
2 Faculty of Medicine, Department of Biochemistry, Dokuz Eylul University, Izmir, Turkey.
*Corresponding Author
Hale Aksu Erdost, MD,
Anesthesiology, School of Medicine,
Dokuz Eylul University, 35340, Izmir, Turkey.
Tel: +90 232 4122801
Fax: 232 4122846
E-mail: haleaksu78@yahoo.com
Received: September 27, 2016; Accepted: October 22, 2016; Published: October 26, 2016
Citation: Onay V, Erdost HA, Ocmen E, Akan P, Gunenc F, et al., (2016) Day and Night Administration of Sevoflurane Effect of Melatonin Levels in Rats. Int J Anesth Res. 4(10), 343-347. doi: dx.doi.org/10.19070/2332-2780-1600071
Copyright: Erdost HA© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: The aim of this study was to investigate the effects of sevoflurane anesthesia in day/night cycles on melatonin
levels in rats.
Methods: Fifteen-day-old 24 rats were included in the study and randomized into four groups according to anesthetic (sevoflurane or control) and the timing of administration (night phase or day phase). 2.6 % sevoflurane and 6 L.min-1 of oxygen were delivered to rats, between 07:00 pm-01:00 am (night group) and 07:00 am-01:00 pm (day group). After the sacrification of the rats, blood samples were taken and samples were centrifuged and plasma melatonin levels were measured by radioimmunoassay.
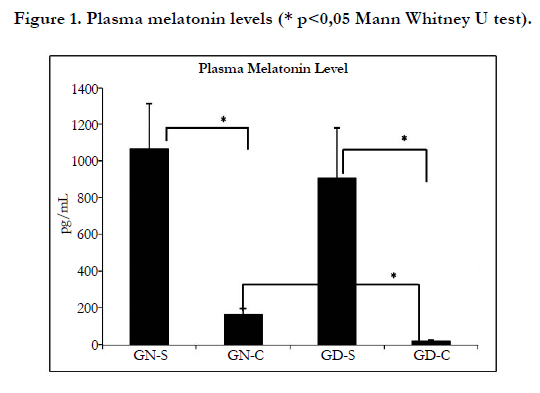
Results: When Group night sevoflurane (GN-S) was compared with Group night control (GN-C), significant difference was found on melatonin levels (p=0,002). When plasma melatonin levels were compared between Group day sevoflurane (GD-S) and Group day control (GD-C), melatonin level of Group Day sevoflurane was found significantly higher (p=0.002). Similarly, when plasma melatonin levels were compared between GN-C and GD-C groups, melatonin level of GN-C was found significantly higher (p=0.002).
Conclusions: In this study, it has been ascertained that 2.6% sevoflurane administered for six hours during the day and night periods increased melatonin levels significantly in 15 days old rats.
2.Introduction
3.Materials and Methods
3.1.Animals
3.2.Drugs
3.3.Experimental Procedures
3.4.Melatonin Measurement
4.Statistical Analysis
5.Results
6.Discussion
7.References
Keywords
Melatonin; Sevoflurane; Anesthesia.
Introduction
Use of general anesthesia to prematures and young children is a part of modern anesthesiology. General anesthetics are usually considered safe, however some recent animal studies allude to anesthetic agents may be harming the immature developing brain. It has been recently shown that frequently used general anesthetics such as benzodiazepines, barbiturates, ketamine, isoflurane and nitrous oxide exposure of the immature rat brain, may cause massive neuronal death [1].
It has been indicated that in anesthesia-induced apoptotic neurodegeneration, mitochondria-dependent apoptotic pathway plays an important role. By up-regulating bcl-XL, which in turn inhibits cytocrome c release and caspase-3 activation, thus blocking the apoptotic cascade activation, melatonin provided a significant neuroprotection (up to 90%) of the developing neurons [2].
Melatonin (N-acetyl-5 methoxytryptamine), is secreted by the pineal gland. The relation between darkness and melatonin secretion indicates the correlation between melatonin, sleep and the circadian rhythm. Neural stimulation from the suprachiasmatic nucleus melatonin secretion varies in response to this stimuli, and it also has receptor-mediated effects on neural and peripheral tissues [3, 4]. Melatonin has several important physiological functions, including regulation of the reproductive axis, regulation of circadian rhythms, oncostatic, antioxidant, anticonvulsant and anti-inflammatory effects [5, 6]. As melatonin has high antioxidant properties, rescuing from both hydroxyl radical and peroxyl radical [7]. Also melatonin has a hypotermic effect, reduces secondary brain damage described in human and animals [8].
A study by Ozkaya et al., [9] showed that isoflurane administration in 15 days old rats at day increased melatonin levels but at night administration made no difference at all.
It’s shown that anesthesia which included fentanyl, atracurium, isoflurane and thiopental, additionally operative stres, can delay the onset of nocturnal melatonin secretion at the first postsurgical evening, leading to sleep disturbances despite adequate pain treatment [10]. Also, it has been examined whether melatonin concentrations can be related with sleep disturbances in seven postoperative patients. Patients received general anesthesia with an inhalation anesthetic during the operation and postoperative pain management provided by an epidural infusion of opioid/ local anesthetic. Nocturnal concentrations of melatonin were found significantly decreased at the first night after surgery [11].
On the other hand, using isoflurane or propofol for general anesthesia was found to increase melatonin plasma levels during daylight hours. After propofol administration for general anesthesia, this change in melatonin levels returned to perioperative baseline levels, whereas melatonin level persisted well into the recovery period in isoflurane group. They hypothesize that altered circulatory melatonin levels may be responsible for the different degrees of postoperative sedation observation in patients [12].
In a series of experiments, Dispersyn et al., [13-15] has shown the propofol anesthesia (without surgery and premedication) affected the circadian pattern of the rest-activity rhythm during the first postanesthesia days in both rats and humans.
The aim of this study was to determine the effect of sevoflurane anesthesia in day or night time on melatonin levels in rats.
Materials and Methods
This present study was conducted in the Multidisciplinary Laboratory of Experimental Animals with the approval of the Board of Ethics in Animal Experiments of Dokuz Eylul University, Faculty of Medicine. All research procedures were performed in agreement with standards and ethics for animal biologic rhythm research [16].
Twenty-four Wistar rats weighing 15 to 20 g ( 2 week old) were housed in individual cages since they were born with food and water available ad libitum, and maintained in a chronobiologic animal facility. The chronobiology facility was equipped with equidistant, sound-proof, temperature-controlled (21°±1.0°C) compartments, each provided with independent light-dark cycles. Rats were maintained for two weeks in a 12-h light/12-h dark cycle (L/D 12:12) before the start of the experiment.
The minimum alveolar concentration for sevoflurane was determined with previous published data obtained for young rats [17]. Oxygen was delivered using a calibrated flowmeter. Sevoflurane was delivered using an agent-specific vaporizer that delivered a set percentage of anesthetic in to the chamber.
Rats were randomly divided into four groups (n=6 animals per group).
Group Night - Control (GN-C) (n: 6): Subjects were given oxygen at 6 L.min-1 from 19:00 to 01:00.
Group Night - Sevoflurane (GN-S) (n: 6): Subjects were given 2.6 % sevoflurane in oxygen at 6 L.min-1 from 19:00 to 01:00.
Group Day - Control (GD-C) (n: 6): Subjects were given oxygen at 6 L.min-1 from 07:00 to 13:00.
Group Day -Sevoflurane (GD-S) (n: 6): Subjects were given 2.6 % sevoflurane in oxygen at 6 L.min-1 from 07:00 to 13:00.
Separate 450 ml glass jars equipped with gas inlet and outlet systems were used for each of the animal. 2.6 % sevoflurane (Sevorane, Abbott Lab. England) in oxygen at 6 L.min-1 concentration of flow rate was given with vaporizer to the glass jars.
In maintenance of anesthesia, the inspired oxygen and sevoflurane concentrations were kept constant by regularly tracing at the anesthetics gas monitor (Anesthesia Gas Monitoring 1304, Denmark) connected to the common inlet line and all the jars were placed in a water bath at a constant temperature of 37°C. All the experimental animals were left to inhale the gas mixture in the jars for a period of six hours.
Rats were kept in the dark during the experimental period in order to protect the subjects of the night groups from light. Red light which rats cannot see was used while collecting blood samples. At the end of the six-hour period, sevoflurane administration to the subjects in the sevoflurane group was terminated and subsequently the subjects’ thoraxes were opened and 1-3 ml blood samples were taken from left ventricles to the eppendorf tubes. Samples were delivered to the laboratory at cold chain. All rats were sacrificed after blood samplings.
Subjects in the control group were given oxygen at 6 L.min-1 throughout the six hours in jar. At the end of this period, rats were sacrificed by cervical dislocation method and immediately their thoraxes were opened, 1-3 ml blood samples were collected from left ventricles into eppendorff tubes and transferred to the lab at cold chain.
In the laboratory, blood samples were centrifuged at +4°C (Hettich Zentrifugen Mikro 22 R, Tuttlingen, Germany) for 15 minutes. Plasma were pipetted into eppendorff tubes and kept at -800°C until assay. Melatonin was tested with Rat Melatonin Radioimmunoassay (RIA) kit (Melatonin Research, RIA, Labor Diagnostica Nord GmbH, England) using the radioimmunoassay (RIA) method at the laboratory of Department of Biochemistry, Faculty of Medicine, Dokuz Eylul University.
Statistical Analysis
Statistical analysis was performed using SPSS for Windows statistical program, version 15.0. Results were given as mean ± standard error form. In the statistical analysis of melatonin values; Levene's test was used for homogenity of group variances, and the distribution was considered homogeneous with values of p > 0.05. Regarding between-group comparisons, t-test was used, and when distribution is not homogeneous Mann-Whitney U test was used. p < 0.05 was considered statistically significant.
Results
24 Wistar rats at ages 15 day and weighing between 15-20 g were included in the study.
In comparison of Group N-S and Group N-C in terms of plasma melatonin levels; Group N-S plasma melatonin values were determined significantly higher (p=0.002). Similarly, when Group D-S and Group D-C were compared, plasma melatonin levels of Group D-S were found significantly higher (p=0.002). Group N-C and Group D-C were also compared with regard to plasma melatonin levels, and Group N-C displayed statistically significant higher levels (p=0.002). On the other hand, when Group N-S and Group D-S were compared, statistically significant difference was not detected between them regarding plasma melatonin levels (p=0.678) (Figure 1).
Discussion
In the present study, we observed 2.6 % sevoflurane administered to 15-day old rats for six-hours during day and night time periods increased plasma levels of melatonin. Our results were similar to the results achieved by Reber et al., [12] and Castro et al., [18] measured melatonin secretion at high levels throughout propofol infusion which was administered for sedation during spinal anesthesia, whereas Reber et al., [18] shown that in the recovery period propofol and isoflurane anesthesia revealed elevated plasma melatonin levels. They said that this elevation gradually decreased in patients anesthetized with propofol, but persisted in patients anesthetized with isoflurane. Contrariwise, Karkela et al., [10] reported that during the first postoperative evening when compared with the preoperative evening, both general and spinal anesthesia significantly decreased melatonin secretion.
Similarly, in another study, patients who had hysterectomy were administered inhalational anesthetic under general anesthesia, and afterwards epidural opioid or local anesthetic to ensure adequate analgesia. These patients were shown to have decreased level of melatonin in the first postoperative night, additionally, serum melatonin levels were higher in the postoperative second and third days compared to the postoperative first day. According to the investigators, the low amplitude of melatonin secretion seen on the first night might be due to unavoidable sleep disturbances in the postoperative period [11].
Fassoulaki et al., [19] applied single sevoflurane short-term anesthesia to 13 adult women who were prepared for cervical dilatation and uterine curettage, and reported no significant change in plasma melatonin and β-endorphin levels of the patients up to 24 hours after surgery. These results may be due to the minor surgery, which is not a painful procedure and is relevant with only minor surgical stress.
In a study conducted with children (aged between 2 and 14 yr.), plasma concentrations of melatonin were reported almost the same levels until after 20 minutes of thiopental sodium or midazolam administrations during ambulatory surgical procedures [20].
In the perioperative period these conflicting results on melatonin secretion, might be due to the dissimilarity in the methodology of measurement of melatonin concentration, differences in anesthetic techniques, or in the duration or complexity of surgical procedures, and other pharmacological interventions during the perioperative period.
Melatonin secretion is known to be affected by the presence and intensity of the light in the environment, and exhibits a marked circadian rhythm [21]. In our study, we wanted to examine the effect of day-night rhythm of anesthesia on plasma melatonin levels. Consequently, without performing any surgical procedure, rats were given sevoflurane at day and night rhythm while breathing spontaneously.
Reber et al., [12] reported that darkness created by administrating anesthesia during the day may cause an increase in the level of melatonin. In our study, the increase in plasma melatonin levels detected at daytime administrations of sevoflurane can be explained by the release of melatonin at the dark atmosphere created by daytime administrations of anesthesia, which eventually result in the increased levels of plasma melatonin.
Our study data regarding increased levels of plasma melatonin due to the application of sevoflurane night and day was found conflicting with the data of Arai et al., [22]. In their study, Arai et al., [22] applied anesthesia induction in women, and reported increased levels of melatonin by isoflurane administration, while decreased levels of melatonin in the use of sevoflurane. The reason may be that, sevoflurane was used only for 5 min during the induction, while 2.6 % sevoflurane was used for six hours in our study. Based on their study data, they reported that circulating melatonin concentration might be increased as a result of an increase in the sympathetic nervous excitation by isoflurane, unlike sevoflurane. In addition, they emphasized that GABAergic transmission, which can affect the synthesis of melatonin, may be altered towards different directions with these two inhalation agents. Analogously Ozkaya et al., [9] reported isoflurane administration in rats at day increased melatonin levels.
Mihara et al., [23] has recently shown administration of ketamine have different effect on melatonin secretion and also on locomotor activity, depending on the time of the administration, whereas penobarbital has no effect. Their hypothesis was based on the most of the anesthetics target GABAA or NMDA receptors, which are found in suprachiasmatic nucleus of hypothalamus. They hypothesis that ketamine as an NMDA receptor antagonist and pentobarbital as a GABAA receptor agonist probably have different effects on the circadian rhythms. Recent studies have shown that volatile anesthetics are equipotent effects on NMDA glutamate signaling. Hollmann et al., [24] showed clinically relevant concentrations of volatile anesthetics such as sevoflurane, isoflurane and desflurane, inhibit functioning of glutamate receptors (NMDA subunits) expressed recombinantly in xenopus oocytes. For determine the effects of these three volatile anesthetics on NMDA receptor signaling, they activated recombinantly expressed NR1/NR2A and NR1/NR2B receptors by co-application of glycine and glutamate in the presence of three volatile anesthetics in three different concentrations. Their results showed all three volatile anesthetics inhibited NMDA receptor signaling dose-dependent, reversible and equipotent. Therefore we thought that as a volatile anesthetic sevoflurane effected NMDA receptor signaling and like ketamine it showed its effect on circadian rhythm. Thus have influence on melatonin secretion. In our study, we observed plasma melatonin levels increased significantly more with sevoflurane administrations at night compared to the night control group, which demonstrated that sevoflurane can increase secretion of melatonin.
In our control group rats, serum mean melatonin levels were determined as 164, 8±31, 41 pg.mL-1 in the night group, while as 17, 83±5, 83 pg.mL-1 in the day group, as it was normally expected for melatonin to exhibit lower serum levels in day groups compared to night groups. In the study of Nowak et al., [25] conducted with rats, the mean serum melatonin level was similarly found 6 pg•mL-1 at daylight applications, while 75 pg•mL-1 at night applications.
In another study of 12 hr light /12 hr dark cycles, even though blood collection time was not clearly noted, melatonin levels were found as 10 pg.mL-1 at daylight, and 45 pg.mL-1 at night applications [26]. Serum melatonin levels were reported as 60 pg.mL-1 in the middle of the night cycle (at 01:30) in rats (19 hours day/5 hours night cycles). All these study data correlated well with our study data.
Rats are nocturnal animals. Their activity cycles coincide with the dark periods, and their maximal activity is correlated with peak levels of melatonin. In humans, this period happens upon sleep so we can not exactly correlate with the human, but most of the anesthesia practice time for human is maximal activity time like rats. Therefore, our study data obtained with rats could be applied to human plasma melatonin [25].
There are some limitations in our study. Among these; monitoring plasma melatonin levels for a limited period of time, and lack of cortisol measurements, which is recognized as the stress hormone and may affect synthesis and secretion of melatonin, are to be mentioned.
Sevoflurane anesthesia administered during day and night was shown to affect melatonin secretion in the rats kept in light-dark (12 h/12 h) cycles for the first time in our study. From the clinical perspective; melatonin may be considered responsible from pathophysiological changes due to plasma level increases that may occur as a result of deterioration of circadian rhythm with sevoflurane and any anesthesia applications independent from surgical procedures.
As a result of this study, conducted with fifteen days old rats, we found sevoflurane administered at 2.6% concentrations in sixhour periods of day and night may increase melatonin. Further studies are required for investigating the effects of general anesthetics on melatonin levels, and as a consequence, on other organs.
References
- Jevtovic-Todorovic V, Hartman RE, Izumi Y, Benshoff ND, Dikranian K, et al., (2003) Early exposure to common anesthetic agents causes widespread neurodegeneration in the developing rat brain and persistent learning deficits. J Neurosci. 23(3): 876-82.
- Yon JH, Carter LB, Reiter RJ, Jevtovic-Todorovic V (2006) Melatonin reduces the severity of anesthesia-induced apoptotic neurodegeneration in the developing rat brain. Neurobiol Dis. 21(3): 522-30.
- Brzezinsk A (1997) Melatonin in humans. N Engl J Med. 336(3): 186-95.
- Reiter RJ, Rosales-Corral S, Coto-Montes A, Boga JA, Tan DX, et al., (2011) The photoperiod, circadian regulation and chronodisruption: the requisite interplay between the suprachiasmatic nuclei and the pineal and gut melatonin. J Physiol Pharmacol. 62(3): 269-74.
- Naguib M, Gottumukkala V, Goldstein PA (2007) Melatonin and anesthesia: a clinical perspective. J Pineal Res. 42(1): 12–21.
- Hardeland R (2005) Antioxidative protection by melatonin: multiplicity of mechanisms from radical detoxification to radical avoidance. Endocrine. 27(2): 119-30.
- Pieri C, Marra M, Monari R, Rechioni R, Marchselli F (1994) Melatonin: A peroxyl radical scavenger more potent than vitamin E. Life Sci. 55(15): 271-276.
- Viswanathan M, Laitinen JT, Saavedra JM (1993) Vasculer melatonin receptors. Biol Signals 2(4): 221-7.
- Ozkaya F, Ocmen E, Akan P, Calan O, Ergurz S, et al., (2013) Day vs. Night Administration of Isoflurane Affects Plasma Melatonin Levels in Rats. Turk J Anaesth Reanim. 41: 111-4.
- Karkela J, Vakkuri O, Kaukinen S, Huang WQ, M Pasanen (2002) The influence of anaesthesia and surgery on the circadian rhythm of melatonin. Acta Anaesthesiol Scand. 46(1): 30-6.
- Cronin AJ, Keifer JC, Davies MF, King TS, Bixler EO (2000) Melatonin secretion after surgery. Lancet. 356(9237): 1244-5.
- Reber A, Huber PR, Ummenhofer W, Gürtler CM, Zurschmiede C, et al., (1998) General anaesthesia for surgery can influence circulating melatonin during daylight hours. Acta Anaesthesiol Scand. 42(9):1050-6.
- Dispersyn G, Pain L, Touitou Y (2009) Circadian disruption of body core temperature and rest-activity rhythms after general (propofol) anesthesia in rats. Anesthesiology. 110(6): 1305–15.
- Dispersyn G, Pain L, Touitou Y (2010) Propofol anesthesia significantly alters plasma blood levels of melatonin in rats. Anesthesiology. 112(3): 333-7.
- Dispersyn G, Touitou Y, Coste O, Jouffroy L, Lleu JC, et al., (2009) Desynchronization of daily rest-activityrhythm in the days following light propofol anesthesia for colonoscopy. Clin Pharmacol Ther. 85(1): 51–5.
- Portaluppi F, Touitou Y, Smolensky MH (2008) Ethical and methodological standards for laboratory and medical biological rhythm research. Chronobiol Int. 25(6): 999 –1016.
- Kashimoto S, Furuya A, Nonaka A, Oguchi T, Koshimizu M, et al., (1997) The minimum alveolar concentration of sevoflurane in rats. Eur J Anaesthesiol. 14(4): 359-61.
- Castro MR, Pastor AB, Alcantud JF, Salvan JH, Osada IR, et al., (2007) Altered plasma melatonin concentrations after administration of propofol in continuous infusion. Rev Esp Anestesiol Reanim. 54(8): 469-74.
- Fassoulaki A, Kostopanagiotou G, Meletiou P, Chasiakos D, Markantonis S (2007) No change in serum melatonin, or plasma beta-endorphin levels after sevoflurane anesthesia. J Clin Anesth. 19(2): 120-4.
- Munoz-Hoyos A, Heredia F, Moreno F, García JJ, Molina-Carballo A, et al., (2002) Evaluation of plasma levels of melatonin after midazolam or sodium thiopental anesthesia in children. J Pineal Res. 32(4): 253-6.
- McIntyre IM, Norman TR, Burrows GD, Armstrong SM (1989) Human melatonin suppression by light is intensity dependent. J Pineal Res. 6(2): 149-56.
- Arai YC, Ueda W, Okatani Y, Fukaya T, Manabe M (2004) Isoflurane increases, but sevoflurane decreases blood concentrations of melatonin in women. J Anesth. 18(3): 228-31.
- Mihara T, Kikuchi T, Kamiya Y, Koga M, Uchimoto K, et al., (2012) Day or Night Administration of Ketamine and Pentobarbital Differentially Affect Circadian Rhythms of Pineal Melatonin Secretion and Locomotor Activity in Rats. Anesth Analg. 115(4): 805–13.
- Hollmann MW, Liu H, Hoenemann CW, Liu W, Durieux ME (2001) Modulation of NMDA Receptor Function by Ketamine and Magnesium. Part II: Interactions with Volatile Anesthetics. Anesth Analg. 92(5): 1182–91.
- Nowak JZ, Zawilska JB (1998) Melatonin and its physiological and therapeutic properties. Pharm World Sci. 20(1): 18-27.
- Yu HS, Reiter RJ (1993) Melatonin: biosynthesis, physiological effects, and clinical applications. CRC Press Inc, USA. 130-45.





