Anesthetic Management in a Patient with Congenital Insensitivity to Pain Syndrome for Lower Extremity Surgery
Akdoğan A, Eroğlu A*, Kutanis D, Cekic B
Karadeniz Technical University, Anesthesiology and Intensive Care Medicine, Trabzon, Turkey.
*Corresponding Author
Ahmet Eroglu,
Karadeniz Technical University,
Anesthesiology and Intensive Care Medicine, Trabzon, Turkey.
E-mail: aheroglu@hotmail.com
Received: July 04, 2016; Accepted: October 13, 2016; Published: October 18, 2016
Citation: Akdoğan A, Eroğlu A, Kutanis D, Cekic B (2016) Anesthetic Management in a Patient with Congenital Insensitivity to Pain Syndrome for Lower Extremity Surgery. Int J Anesth Res. 4(10), 340-342.doi: dx.doi.org/10.19070/2332-2780-1600070
Copyright: Eroğlu A© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Congenital insensitivity to pain (CIP) is a rarely syndrome and is characterized by unresponsiveness to painful stimulants, anhydrous, mental retardation, and recurring feverish episodes. In this case report we presented our anesthesia management in a patient with congenital insensitivity to pain for lower extremity surgery due to osteomyelitis.
2.Introduction
3.Case Presentation
4.Discussion
5.Conclusion
6.References
Keywords
Congenital Insensitivity to Pain (CIP) Syndrome; Anesthesia; Lower Extremity Surgery.
Introduction
Congenital insensitivity to pain (CIP), first described by Dearborn in the year 1932, is a rarely encountered neuropathic syndrome that manifests itself starting from birth and is characterized by unresponsiveness to painful stimulants, anhydrous, mental retardation, and recurring feverish episodes [1].
The cases usually involve painless fractures, finger, lip and tongue injuries, neurogenic arthropathies (Charcot joint), and joint deformities that could lead to chronic osteomyelitis [2]. The mortality rate of the disease is very high due to the fact that there is no specific treatment that could be administered. The subjects are usually deceased by the time they reach their adolescence.
In cases where the subjects are required to go through a surgical procedure, in spite of the fact that the patient is unresponsive to pain, it would still be necessary to administer anesthesia to prevent unwanted circumstances such as tactile hyperesthesia.
We would like to present our experiment regarding anesthesia management under Bispectral index (BIS) monitoring in a patient with congenital insensitivity to pain for lower extremity procedure due to osteomyelitis.
Case Presentation
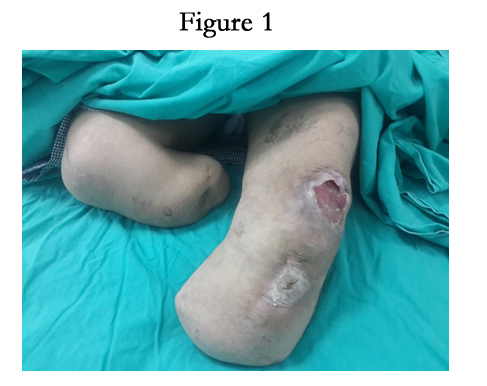
The plastic surgery clinic planned to operate on a 16 year old 60 kg male patient in ASA II group suffering from congenital insensitivity to pain and diagnosed previously with osteomyelitis development in the left patellar region (Figure 1). In the preoperative assessment of the patient, the laboratory values and lungs were normal. The patient, who was subjected to physical examination, was insensitive to pain and temperature and displayed slight mental retardation. His other neurologic examination results and his sense of touch were normal. The airway evaluation revealed Mallampati classification to be III and sternomental distance to be 10 cm, while the neck movements were determined to be restricted.

Prior to the procedure, the patient’s family members were informed of the anesthesia method to be applied and the potential risks and their consent was obtained.
Fiberoptic bronchoscope, laryngeal mask and tubes of various sizes were kept handy to encounter any difficulties that could be experienced with the airway of the patient.
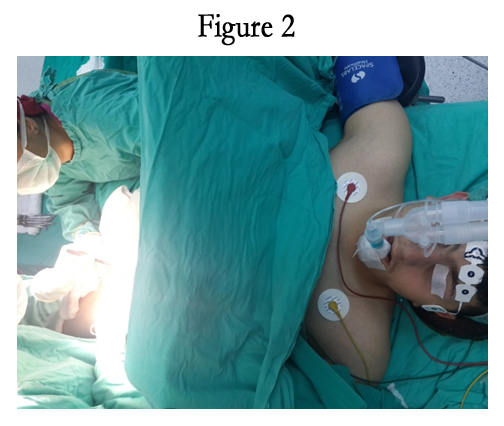
The fluid infusion was started with a 24G cannula applied on the back of the left hand of the patient after he was moved into the operating room. As premedication the patient was later on administered 0.05 mg/kg midazolam as bolus IV. The standard monitoring of the patient was conducted by means of electrocardiography, non-invasive arterial blood pressure and pulse oximetry. Additionally axillary temperature monitoring and BIS monitoring (BIS, VISTA Monitoring System, USA) were conducted (Figure 2). The measurements obtained from the monitoring were as follows: pulse rate 79 beats/min, blood pressure 130/58 mmHg, SpO2 99, temperature 36.7, BIS 92.

Following the administration of 3 mg/kg propofol as bolus IV, the No. 4 laryngeal mask was placed on the patient with BIS 40 without any problems in the first attempt. His cuff was inflated with 10 ml air. The listening of the lungs showed them to have received equal and sufficient air. The anesthesia maintenance was administered as a mixture of 50% O2 + 50% air and propofol infusion of 2-5 mcg\kg\h as BIS was maintained between 40 and 60. The temperature in the operating room was maintained in a range of 22-24 degrees.
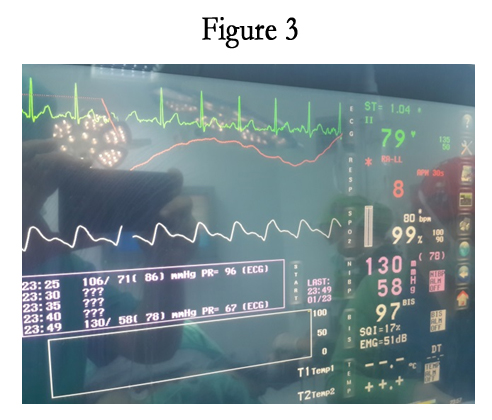
During the procedure, 0.5 mg atropine sulphate was administered as heart rate was first 45/min then 30/min. During this time period, the arterial blood pressure values were normal (Figure 3). As we approached the end of the surgical procedure that took about 30 minutes the propofol infusion was stopped and the respiration was switched to 100% O2. The laryngeal mask of the patient, whose spontaneous respiration was observed to be sufficient and regular, was removed without any problems after he opened his eyes (BIS Value 85) and was able to lift up his head (BIS value 90). There was no need to administer additional anesthetic or analgesic agents to the patient during the intraoperative period.
In the Post Anesthesia Care Unit (PACU), 4 lt/min O2 was administered through mask during the 30-minute follow-up period. The patient was sent to the plastic surgery service as his arterial blood pressure was determined to be 115/75 mmHg, heart rate 85 beats/min., peripheric O2 saturation 99%, and body temperature 37.3 degrees. The patient, who did not require analgesics in the service follow-up either, was discharged after 5 days.
Discussion
Congenital insensitivity to pain (CIP) is an autosomal recessive disorder that is characterized by fever episodes that are secondary to anhydrous, varying degrees of mental retardation, and absence of pain and consequently self inflictedinjuries. This is a rarely encountered disorder with only 300 reported cases across the world [3].
Some of the significant manifestations of CIP are the anomalies in the sense of heat, whereas the sense of touch is not normal and there is insensitivity to superficial and deeper painful stimulus. Furthermore, the deep tendon reflexes are hypoactive or non-existent and the patients display varying degrees of mental retardation [4].
Although the cardiovascular reflexes are maintained, the patients could develop serious hypotension in the perioperative period due to the diminishing levels of catecholamine and most distinctly due to the fact that it affects norepinephrine and epinephrine levels. That being said, our subject developed bradycardia twice. The progress of the bradycardia was prevented by administering atropine sulphate.
In Congenital insensitivity to pain, the body temperature control is disrupted due to systemic anhydrous which causes episodes of sudden temperature hikes. For this reason, 20% of people suffering from this disorder lose their lives within the first 3 years after birth [5]. As a matter of fact, our patient also reported to have suffered frequent attacks of fever. In addition to temperature control, control of the ambient temperature, and use of the heating and cooling blankets could be employed to control the body temperature changes intraoperatively. We monitored the body temperature of our subject through intraoperative axillary temperature monitoring.
During a surgical procedure, in spite of the fact that the patients are unresponsive to pain, it would still be necessary to administer anesthesia due to the fact that tactile hyperesthesia could develop. Administration of general anesthesia eliminates any fear and anxiety in patients with mental retardation like in our case, as well as preventing the formation of new fractures as it ensures the patient remains immobile. It could be observed upon examination of the literature that in majority of the cases, general anesthesia [5, 6] is preferred though there were also cases where sedation was the selected method [7, 8]. Although administration of general anesthesia has many advantages, in cases where the catecholamine levels are diminishing, it could cause serious hypotension [4].
The medications that could be administered to CIP patients without any adverse effects are atropin, meperidine, fentanyl, succinylcholine, atracurium, pancuronium, vecuronium, ketamine, propofol, pentothal and benzodiazepine [6]. We used propofol infusion with 50% air + 50% O2 without any problems in our case.
It is very important that the level of administered anesthesia is determined and maintained to achieve sufficiently deep anesthesia. To serve this purpose we used Bispectral index (BIS) device in our case. By means of BIS monitoring that is employed intraoperatively, the dosage and timing of the anesthetic agents administered with the depth of anesthesia displayed can be determined and the early recovery of consciousness could be prevented [9]. The values between 40-60 on BIS are indicative of consciousness at its lowest level in subjects under surgical stimulants. We also considered values between 40-60 as our reference points in measuring how deep the level of anesthesia was.
Conclusion
In cases of CIP where surgical intervention is necessary, it is definitely necessary to administer anesthesia to avoid tactile hyperesthesia. We are of the opinion that in addition to standard monitoring of anesthesia, monitoring of the temperature, measuring the depth of the administered anesthesia and conducting BIS monitoring to prevent consciousness could prove to be beneficial.
References
- Dearborn G (1932) A case of congenital pure analgesia. J NervMent Dis. 75: 612-615.
- Terada Y, Furuya A, Ishiyama T, Matsukawa T, Kumazawa T (2001) Anesthetic management of a child with congenital sensory neuropathy with anhydrosis. Masui. 50(7): 789-791.
- BAR-On E, Weigl D, Parvari R, Katz K, Weitz R, et al., (2002) Congenital insensitivity to pain orthopaedic manifestations. J Bone Joint Surg Br. 84(2): 252-257.
- Okuda K, Arai T, Miwa T, Hiroki K (2000) Anaesthetic management of children with congenital insensitivity to pain with anhidrosis. Paediatr Anaesth. 10(5): 545-548.
- Oliveira CR, Paris VC, Pereira RA, Lara FS (2009) Anesthesia in a patient with congenital insensitivity to pain and anhidrosis. Rev Bras Anestesiol. 59(5): 602-609.
- Tomioka T, Awaya Y, Nihei K, Sekiyama H, Sawamura S, et al., (2002) Anesthesia for patients with congenital insensitivity to pain and anhidrosis: a questionnaire study in Japan. Anesth Analg. 94(2): 271-274.
- Layman PR (1986) Anaesthesia for congenital analgesia. A case report. Anaesthesia. 41(4): 395-397.
- Kılıçaslan A, Gök F, Yaşar E, Başdemirci A, Otelcioğlu, Ş (2014) Konjenital Ağrı Duyarsızlığı Sendromunda Bispektral İndeks Rehberliğinde Sedasyon Uygulaması. Turk J AnaesthReanim. 42: 292-293.
- Sleigh JW, Donovan J (1999) Comparison of bispectral index, 95% spectral edge frequency and approximate entropy of the EEG, with changes in heart rate variability during induction of general anaesthesia. Br J Anaesth. 82(5): 666-671.





