Acromegaly,Endocrine Dysfunction and Polyostotic Fibrous Dysplasia Associated With Mccune-Albright Syndrome: Anesthetic Considerations Case
Moran K1*, Agbenyefia P2, Mani M 1, Bergese S1,3, Stoicea N1
1 Department of Anesthesiology,Wexner Medical Center, Ohio State University, Columbus, OH, USA.
2 College of Medicine, The Ohio State University, Columbus, OH, USA.
3 Department of Neurological Surgery, Wexner Medical Center, Ohio State University, Columbus, OH, USA.
*Corresponding Author
Kenneth Moran,
Assistant Professor
Clinical, Residency Program Director,
Department of Anesthesiology,
The Ohio State University Wexner Medical Center,
Columbus, OH, USA
Tel: (614) 293-8487;
Fax: (614) 366-8535
E-mail: kenneth.moran@osumc.edu
Article Type: Case Report
Received: June 12, 2014; Accepted: June 27, 2014; Published: June 30, 2014
Citation: Agbenyefia P, Mani M, Bergese S, Stoicea N, Moran K (2014) Acromegaly, Endocrine Dysfunction and Polyostotic Fibrous Dysplasia Associated With Mccune-Albright Syndrome: Anesthetic Considerations. Int J Anesth Res. 2(4), 45-47. doi: http://dx.doi.org/10.19070/2332-2780-1400012
Copyright: Moran K© 2014 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
McCune-Albright Syndrome is a rare disorder affecting the skin, bones and endocrine tissues. It is characterized by the presence of café au lait spots, polyostotic fibrous dysplasia, and autonomous endocrine hyperfunction. Perioperative management of patients with this syndrome is frequently complex, as they are prone to a large array of comorbidities including pathologic fractures and spinal instability, acromegaly, hyperthyroidism, hypophosphatemia, Cushing’s syndrome and chronic systemic hypertension, liver disease, and arrythmias. Anesthesiologists are faced with a spectrum of challenges in the perioperative management of these patients. Macroglossia and macrognathia can result in airways which are difficult to visualise and secure. Frail bones and spinal instability often complicate positioning, and endocrinopathies may result in an increased propensity for cardiac arrhythmias perioperatively. The objective of this paper is to report the case of a 36 year-old male with McCune-Albright Syndrome presenting for a T10-11 laminectomy due to spinal cord compression and to discuss our management of this complicated patient with a history of hypophosphatemia, scoliosis, multiple long bone fractures, non-ischemic cardiomyopathy, atrial fibrillation, and severe acromegaly from a growth hormone-secreting pituitary adenoma.
2.Introduction
3.Case Report
4.Discussion
5.Conclusion
6.References
Keywords
McCune Albright Syndrome; Polyostotic Fibrous Dysplasia; Acromegaly; Anesthesia; Endocrinopathies.
Introduction
McCune-Albright Syndrome (MAS) is a genetic disorder characterized by the presence of at least two of three features of the classic traid of polyostotic fibrous dysplasia, hyperpigmented skin patches (café au lait spots), and endocrine hyperfunction. The worldwide prevalence of MAS is 0.1-1 per 1,000,000 [1,5]. MAS is caused by sporadic, gain-of-function mutations in the GNAS gene, which codes for the stimulatory G-protein alpha subunit [2]. This leads to constitutive activation of adenylate cyclase and overproduction of cAMP in the tissues deriving from the embryonic cell in which the mutation occurred. Thus, the severity and clinical picture of MAS vary based on which cells possess the mutated GNAS gene [2].
Polyostotic fibrous dysplasia and cafe-au-lait spots are the most frequent presenting features of the classic triad, occurring in 46% to 98% and 53.1% to 92.5% of patients respectively [5,6,10]. Patients with MAS who present with polyostotic fibrous dysplasia have fibrous bone lesions as a result of abnormal bone remodeling and demineralization [2,5]. Radiologically, these bones may have endosteal scalloping, thin cortex, and an intramedullary tissue matrix showing a ground glass appearance [5]. Replacement of bone with fibrous tissue predisposes patients to pathologic fractures, uneven growth, and deformities [2].
Endocrinopathies associated with MAS include acromegaly, hyperthyroidism, hyperprolactinemia, ACTH-independent hypercortisolism, and precocious puberty from ovarian hypersecretion of estradiol. Precocious puberty is the most common presenting endocrinopathy among patients with MAS [5]. It is seen in 64% to 79% of cases, is more common in women [5], and has been diagnosed as early as age 22. In one case series, 57% of pediatric cases reviewed had precocious puberty [9].
Acromegaly is usually diagnosed in early or mid adulthood [9]. It affects around 21% of MAS patients [3,7], and is a consequence of excess growth hormone from a growth hormone secreting pituitary adenoma after metaphyseal fusion. Acromegaly in MAS is almost always associated with skull-base fibrous dysplasia [9], and has been accompanied by various craniofacial malformations [5] as well as macrocephaly. It is also associated with macroglossia and macrognathia. Hyperprolactinemia is also a common finding, with a prevalence of 85% in patients with MAS and acromegaly [3]. Acromegaly in MAS patients is usually difficult to treat although somatostatin analoques and D2 agonists have shown promising results [8].
Hyperthyroidism has been reported in 38% of MAS cases [7] and is generally due to multinodular toxic goiter [8]. This can be particularly roblematic in a postoperative setting since uncontrolled hyperthyroidism confers increased risk for thyroid storm. A number of cases of postoperative thyroid storm have been reported in MAS patients, usually within 6 to 18 hours of surgery [4]. The presence of endogenous Cushing’s syndrome may also call for careful monitoring, as patients are often hypertensive, hyperglycemic and hypokalemic. It is critical for anesthesiologists to be cognizant of the type and severity of endocrinopathies in patients with MAS, to be prepared for anatomical limitations to airway management, and to be aware of the condition of their cervical spine and other bony abnormalities that could contribute to position related morbidity.
Case Report
A 36 year-old male with McCune-Albright Syndrome and spinal cord compression presented for a T10-11 laminectomy. His medical history included severe acromegaly, growth hormoneand prolactin-secreting pituitary adenoma, scoliosis, C3 vertebroplasty, multiple long bone fractures, hypophosphatemia, non-ischemic cardiomyopathy, and atrial fibrillation. His home medications included levothyroxine, bromocriptine, pegvisomant, sandostatin, delatestryl, potasium phosphate, zoledronate, calcium carbonate, calcitriol, oxycodone, aspirin, metoprolol and lisinopril. Physical exam findings revealed right-sided blindness and deafness, enlarged mandible, prominent tongue, and cervical instability with significantly decreased neck extention and overall range of motion. Airway visualization demonstrated a Mallampati IV classification. The lungs were clear to auscultaiton bilaterally, and cardiac exam was positive for an irregularly irregular rate and rhythm. Oral fiber optic intubation was easily performed and a #8 endotracheal tube was passed through a large glottic opening. It was noted that once the fiberoptic scope was passed beyond the large jaw and tongue, the periglottic space was large and unobstructed. Propofol induction and maintenance with desflurane, remifentanyl and dexmedetomidine proceded uneventfully. Special precautions were taken in positioning the patient as the surgery required prone positioning for an extended period of time. Extra help was recruited to turn the patient to the prone position because of the patient’s large size and potential for cervical spine injury. The large head made it expecially difficult to maintain inline stabilization while turning. While in the prone position, the disproportionate head size required removing the mounts from the head rest so that it could be lowered. This allowed appropriate spinal alignment to avoid cervical strain. The patient’s large head and particularly prominent forehead, from both acromegaly and fibrous dysplasia, made it difficult to achieve neutral cervical alignment, even with alteration of the standard headframe. Additional padding was used for the face, and altered eye goggles were fitted by cutting them above the bridge of the nose to allow for wide eye spacing. The head support was widened by manual force to permit entry of the large head and padding. Pressure points were also padded to avoid nerve compression injury from enlarged and abnormal bony prominences. T10-11 laminectomywas performed successfully, and the patient was extubated fully awake in the operating room without complications.


Figure 1. Picture of patient being fitted with a facemask.

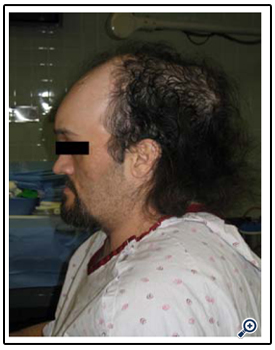
Figure 2. Lateral view of patient demonstrating his large head size with prominent forehead and mandible.
Discussion
McCune-Albright Syndrome is a complex condition that results in multiple challenges for the anesthesiologist. The combination of acromegaly and polyostotic fibrous dysplasia may cause difficulties in safely securing the airway. Airway issues in this particular case included maglossia with a Mallampatti IV airway classification, macrognathia, and poor neck extension due to potential cervical spine instability. Cervical spine instability was attributed to the patient’s large and heavy head, in addition to a history of cervical spine compression fractures previously treated with a C3 vertebroplasty. Careful manipulation of the head is paramount as fibrous dysplasia and resulting dysmorphisms predispose these patients to skull fractures, which can lead to injury of the optic, auditory, or other cranial nerves. The patient was noted to have right-sided blindness and deafness, which were present at presentation. Adequate padding and positioning as well as a widened head support may be necessary to prevent fractures in patients with MAS with acromegaly.
Oral fiber optic endotracheal intubation was performed in this case primarily because of the patient’s cervical instability and out of concern for complications that might arise from manipulation of the neck. The use of direct laryngoscopy in patients with acromegaly requires special care to avoid pathologic fracture of the mandible [1].
Induction and maintenance of general anesthesia can be complicated by arrhythmias and sudden cardiac death due to baseline endocrinopathies in patients with MAS. Chronic hypercorticism may lead to altered cortisol response to stress. As such, it is recommended that MAS patients with Cushing’s syndrome receive perioperative steroids to prevent “adrenal crisis”. [4] The patient in this case had no signs of acute or chronic hypercortisolism or hyperthyroidism. Despite baseline atrial fibrillation in this patient, propofol induction and maintenance with desflurane, remifentanyl and dexmedetomidine was uneventful. Dexmedetomidine was added for its beneficial effects on atrial arrythmias and rate control.
Conclusion
McCune-Albright Syndrome (MAS) is a genetic disorder characterized by the presence of polyostotic fibrous dysplasia, café au lait spots, and endocrine hyperfunction. As demonstrated in this case report, MAS presents anesthesiologists with many obstacles that must be understood and overcome to safely perform anesthesia. For instance, airway management and positioning may be complicated by macroglossia and macrognathia, as well as other craniofacial malformations, cervical spine instability and overall bone fragility due to fibrous dysplasia. A familiarity with baseline endocrinopathies and their level of severity in patients with MAS will ensure appropriate planning and management by the anesthesiologist in the perioperative setting. Special attention to airway management, positioning and endocrinopathies is important to prevent perioperative complications in these patients.
References
- Strauss EJ, Poplak TM, Braude BM (1985) Anesthetic management of a difficult intubation. S Afr Med J;68:414-4
- McCune-Albright syndrome. (2014, April 28). Retrieved May 1, 2014, from http://ghr.nlm.nih.gov/condition/mccune-albright-syndrome
- Almeida, J. P. C, Albuquerque, L. A. F, Ferraz, C. L. H, Mota, Í, Gondim, J, et al (2009) McCune-albright syndrome and acromegaly: hormonal control with use of cabergoline and long-acting somatostatin - case report. Arquivos Brasileiros de Endocrinologia & Metabologia, 53(1), 102–106. doi:10.1590/S0004-27302009000100015
- Langer, R. A, Yook, I, & Capan, L. M (1995) Anesthetic considerations in McCune-Albright syndrome: case report with literature review. Anesthesia and Analgesia, 80(6), 1236–1239.
- Dumitrescu, C. E, & Collins, M. T (2008) McCune-Albright syndrome. Orphanet Journal of Rare Diseases, 3(1), 12. doi:10.1186/1750-1172-3-12
- Rizzo, J. M, Loss, L. C, & Rothman, I. L (2013) Hyperpigmented patches on the neck, shoulder, and back. Cleveland Clinic Journal of Medicine, 80(5), 290–296. doi:10.3949/ccjm.80a.12033
- Salpea, P, & Stratakis, C. A (2014) Carney complex and McCune Albright syndrome: an overview of clinical manifestations and human molecular genetics. Molecular and Cellular Endocrinology, 386(1-2), 85–91.doi:10.1016/j.mce.2013.08.022
- Chanson, P, Salenave, S, & Orcel, P (2007) McCune-Albright syndrome in adulthood. Pediatric Endocrinology Reviews: PER, 4 Suppl 4, 453–462.
- Salenave, S, Boyce, A. M, Collins, M. T, & Chanson, P (2014) Acromegaly and McCune-Albright syndrome. The Journal of Clinical Endocrinology and Metabolism, jc20133826. doi:10.1210/jc.2013-3826
- Aycan, Z, Onder, A, & Cetinkaya, S (2011) Eight-Year Follow-up of a Girl with McCune-Albright Syndrome. Journal of Clinical Research in Pediatric Endocrinology, 3(1), 40–42. doi:10.4274/jcrpe.v3i1.09





