Sildenafil Attenuates Pulmonary Hypertension Following Fat Embolism in an Anaesthetised Rat Model
Gerard Davis2, Thilak Jepegnanam1, Andrew McNaughton3, Mark Walton1, Jean-Claude Theis1*
1 Departments of Surgical Sciences, Dunedin School of Medicine and Otago School of Medical Sciences, University of Otago, Dunedin, New Zealand.
2 Departments of Physiology, Dunedin School of Medicine and Otago School of Medical Sciences, University of Otago, Dunedin, New Zealand.
3 Departments of Anatomy, Dunedin School of Medicine and Otago School of Medical Sciences, University of Otago, Dunedin, New Zealand.
*Corresponding Author
Jean-Claude Theis,
Section of Orthopaedic Surgery,
Department of Surgical Sciences,
Dunedin School of Medicine,
University of Otago,
PO Box 913, Dunedin, New Zealand.
Fax: 64 3 4747617
E-mail: jean-claude.theis@otago.ac.nz
Article Type: Research Article
Received: March 17,2014; Accepted: March 31,2014; Published: April 02, 2014
Citation: Jean-Claude Theis et al (2014) Sildenafil Attenuates Pulmonary Hypertension Following Fat Embolism in an Anaesthetised Rat Model. Int J Anesth Res. 2(3), 40-44. doi: dx.doi.org/10.19070/2332-2780-1400011
Copyright: Jean-Claude Theis© 2014. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Release of fat and bone marrow during medullary pressurisation leads to fat embolism and pulmonary hypertension resulting in serious cardiorespiratory complications.
This study aimed to determine whether pre-treatment with the phosphodiesterase type 5-inhibitor, Sildenafil, prevents pulmonary artery hypertension in an animal model.
The animals either received Sildenafil (5 mg kg-1) or saline intra peritoneally 15 minutes prior to medullary pressurisation with bone cement. Cardiovascular parameters were recorded throughout the procedure. At the end radiopaque contrast was injected into the pulmonary circulation; the lungs were then harvested and imaged using micro CT.
Medullary pressurisation in the control animals caused pulmonary hypertension and systemic hypotension. This was associated with a decrease in the area of perfusion of the lungs. These changes were attenuated by pretreatment with Sildenafil.
We conclude that in this animal model fat embolism causes similar cardiovascular changes as observed in clinical practice and pretreatment with Sildenafil attenuates these effects.
2.Introduction
3.Methods
3.1 Ethics
3.2 Animals
3.3 Experimental Protocol
3.4 Micro CT
3.5 Histology
3.6 Statistical Analysis
4.Results
4.1 PAP
4.2 MAP
4.3 HR
4.4 Micro CT and histology
5.Discussion
6.Acknowledgements
7.References
Keywords
Pulmonary Artery Pressure; Sildenafil; Fat Embolus.
Introduction
Fat is regularly displaced from the medullary cavity during orthopaedic surgery [1] and particularly during fracture treatment or joint replacement.[1] The fat enters the circulation and has profound effects on the cardiorespiratory system, both acutely [2] and secondarily leading to respiratory failure as part of fat embolism syndrome. Previous studies from this research group have shown fat emboli released into the circulation during vertebroplasty, in a sheep model, leading to a rapid decrease in cardiac output and arterial blood pressure, and an increase in pulmonary artery pressure (PAP).[3, 4, 5] The increase in PAP is thought to be a result of the vasoactive properties of the emboli and the mechanical obstruction of the smaller blood vessels in the lungs.[6, 7].
Sildenafil is a selective and potent inhibitor of cGMP specific phosphodiesterase type 5 (PDE5), which is found primarily in the pulmonary circulation, and blocking the action of PDE5 attenuates the breakdown of nitric oxide.[8] Sildenafil treatment initially had FDA approval for the treatment of infants with pulmonary hypertension [9] and is currently being investigated for the use in pulmonary hypertension associated with left heart disease.[10]
Krebs et al [6] using a sheep model, has shown that Sildenafil is effective at reducing PAP following bone augmentation. While a sheep model is a good approximation of the human anatomy, in terms of size of the circulation, lungs etc., there are significant logistical limitations to using large animals. Therefore, the aim of this study was to develop a rat model to measure the cardiovascular effects of pressurisation of both femurs using cement. The major advantages of this model are that it is possible to have one person carry out the surgery and postoperative monitoring, and that it allows a more complete sampling of tissues, unlike in sheep, where only a small sample of tissue is taken, which may lead to selection bias. Using this rat model allows the entire lung to be imaged using micro CT, which wouldn’t be possible in a larger animal.
We hypothesise that pre-treatment with the phosphodiesterase type 5 inhibitor, Sildenafil, will attenuate the pulmonary hypertension resulting from fat embolism following bone pressurisation.
This study was approved by the University of Otago Animal Ethics Committee (AEC 45/07).
Male Sprague-Dawley rats (3-month old, n=12) were fasted overnight but had free access to water. The animals were anesthetised with urethane (1.5 g kg-1, intra peritoneal) and the trachea was instrumented to reduce respiratory complications. The carotid artery was cannulated to measure arterial blood pressure, via a pressure transducer (Statham P23AC, Halo Rey, Puerto Rico) connected to a MacLab 8/s (ADInstruments) via a bridge amplifier (ADInstruments). The output was displayed on a channel of Chart® software (version 5.2 ADInstruments) on a computer. The heart rate was derived from the pulse pressure and displayed on the computer. The left jugular vein was cannulated for infusion of intravenous fluids (150 mM NaCl, 3 ml h-1). The right jugular vein was cannulated with an 3.5 French umbilical vessel catheter and advanced into the pulmonary artery, via the right ventricle. The catheter was connected to a pressure transducer (Delta II, Disposable Pressure Transducer System, Utah Medical Products, USA) and the output was displayed on a second channel of the Chart software.
The left and right femurs were exposed via a medial para-patellar arthrotomy and the patella displaced to one side, thus exposing the femoral condyles. A 1.5 mm drill was used to gain access to the medullary cavity. The animal was allowed to equilibrate prior to baseline data being recorded.
The animals were randomly assigned to either a control (intra peritoneal saline, 2 ml kg-1) group (n=6) or experimental (intra peritoneal Sildenafil 5 mg kg-1) group (n=6). Baseline arterial and pulmonary blood pressure and heart rate were collected for 20 minutes after which a half dose of cement (Simplex cement, Stryker, New Zealand) was injected into the femurs using a tightly fitting 14G needle. After injection, the cement was pressurised by tapping a 1.7 cm long 1 mm diameter wire into the medullary cavity of the femur. The procedure was repeated on the contralateral side. Data was collected for one hour following the end of the procedure. At the end of the data collection, 4 ml of diluted contrast medium (Iohexol 340, 50:50 with saline) was slowly injected into the pulmonary circulation via the pulmonary artery catheter, over a period of 60 seconds. Thirty seconds later the rat was euthanized with an overdose of urethane, via the left jugular vein cannula, and the lungs harvested. The lungs were placed in fresh 4% phosphate buffered formalin and were used for micro CT and histology.
The lungs were partially inflated and suspended by the trachea in a sealed polystyrene container to prevent dehydration. The container was placed on the stage of micro CT (SkyScan 1172 High Resolution X-Ray Micro-Tomograph, SKYSCAN, Kartuizersweg 3B, 2550 Kontich, Belgium) and the lungs were imaged using the following settings: X-ray source 100kV sealed microfocus air-cooled and spot size < 5 μm. The X-rays were detected with a 10 Megapixel (4000 x 2300) 12-bit digital cooled CCD camera, coupled via a fibre optic cable to the scintillator (50 mm field of view). To compensate for beam-hardening we used an automatic filter changer and multi-energy scanning. The image resolution was 17.35 μm and the scan time 38 minutes. NRecon software was used to produce tomographic images of the slices through the lung tissue, and then 3D images were constructed using Amira software (version 4.1.2 Visage Imaging, Wuerzburger Str. 197, D-90766, Fuerth, Germany) using an Apple Macintosh computer (Power Mac with a 2.66 GHz dual-core Intel Xeon processor, running OS X 10.4.11). The file size was reduced to give a final image resolution of 34.7 μm in order to make the images more manageable.
Following imaging with the micro CT the lungs remained in the phosphate buffered formalin for a total of 2 hours. Three 2 mm sections of lung were taken: one sagittal section through the entire left lung, and two coronal sections through the right lung, one through the lower lobe and the other through the middle lobe. Each section was placed in phosphate buffered sucrose solution overnight at 4°C. The sections were then fresh frozen in OCT (TissueTek), using isopentane cooled by liquid nitrogen. The lung tissue was sectioned (20 μm), mounted on glass slides (HistoBond) and stained for the presence of fat, using Oil Red O. The distribution of Oil Red O staining was determined using a microscope (Olympus BX50) and images captured using a digital camera (Spot RT, Diagnostic Instruments, Sterling Heights, MI, USA) and Spot software (version 4.5, Diagnostic Instruments), running on a Computer (Apple Macintosh). The sections were examined at 10x magnification and the total number of fat emboli was counted manually. The area of each section was divided using graph paper and the number of fat emboli per 100 mm2 was determined.
The response to Sildenafil and to bone augmentation between groups was compared using a 2-way ANOVA, with repeated measures, while within group comparisons a 1-way ANOVA with repeated measures was carried out followed by a univariate analysis at each time point to identify values which were different from basal recordings (in the case of a response to Sildenafil or saline) or the 0 minute time point (in the case of the response to bone augmentation). For histology and micro CT control and Sildenafil treated rats were compared using a non-parametric Mann- Whitney test. The software used was JMP 7.02 (SAS, Sydney, Australia).
Results
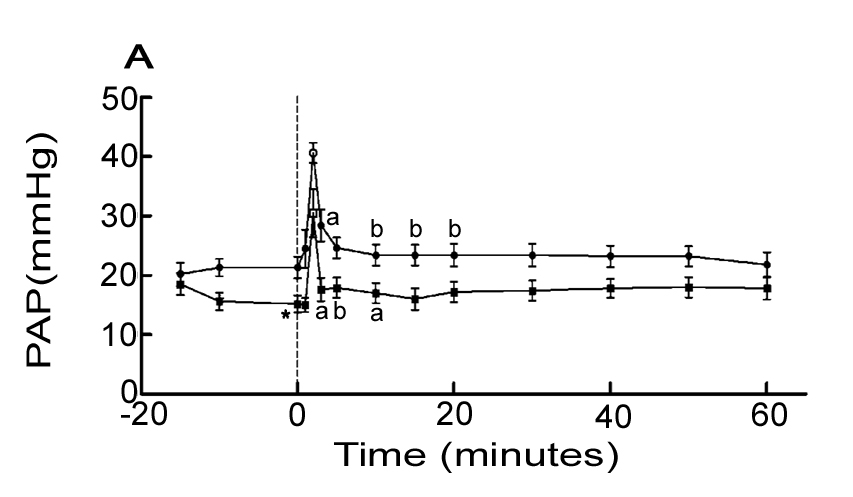
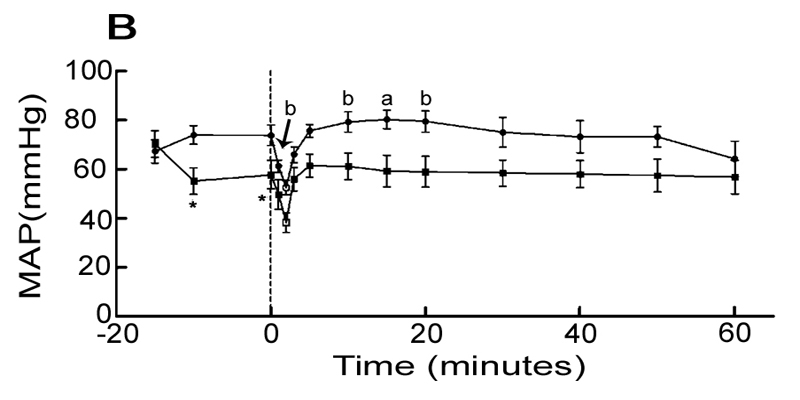
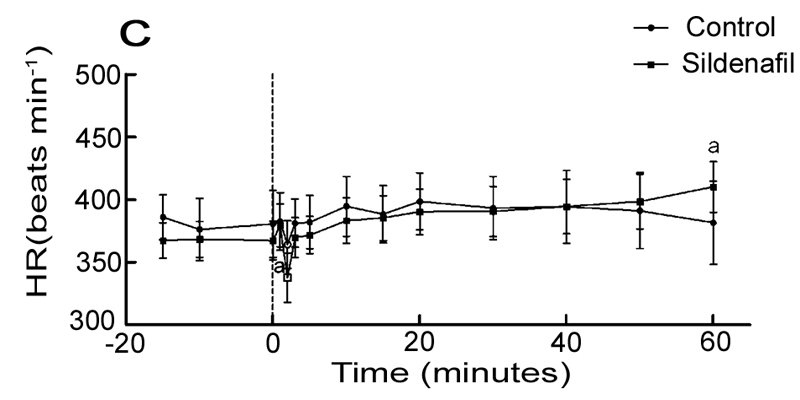
Figure. 1 shows the cardiovascular response to bilateral bone augmentation in control and Sildenafil treated rats.
FIgure 1: Cardiovascular response to bilateral medullary pressurisation in control (n = 6) and Sildenafil (n = 6) treated rats. Abbreviations:Pulmonary Artery Pressure (PAP), Mean Arterial Pressure (MAP) and Heart Rate (HR). Asterisk (*) indicate significant difference from basal; * = p < 0.05. Letters indicate significant difference from time 0; a = p < 0.05; b = p < 0.01.
In the control group there was no change in PAP, MAP or HR prior to bone augmentation. However, in the Sildenafil group, we observed a significant decrease in PAP (p = 0.0007) and MAP (p = 0.0021) as compared to basal values in response to intra peritoneal Sildenafil injection. There was no change in HR.
Injection of Sildenafil resulted in a decrease in PAP by 15 ± 3 mmHg (p = 0.021) and 17 ± 4 mmHg (p = 0.0257) at 5 and 15minutes respectively. This response was significantly different from the saline treated control animals (p< 0.0001).
In the saline group, bone augmentation significantly increased PAP (p = 0.0009) by 36 ± 12% (p = 0.0308) at 3 minutes, and remained elevated for 30 minutes. In the Sildenafil group, while PAP increased by 15 ± 2% (P = 0.0241) at 3 minutes, it remained elevated for 10 minutes only. Overall the PAP response in the Sildenafil group was significantly smaller than the saline control group (p = 0.0205).
Femur pressurisation caused a large transient increase in PAP (figure 1A, open symbols) between 1 and 2 minutes after the cement injection in both saline (40 ± 2 versus 21 ± 2 mmHg, p < 0.0001) and Sildenafil groups (31 ± 4 versus 15 ± 1 mmHg, p = 0.0024), compared to pre-pressurisation values. There was no difference in the magnitude of the response in the two groups.
Sildenafil decreased MAP by 22 ± 4 (p = 0.0162) and 18 ± 6 mmHg (p = 0.0472) at 5 and 15 minutes respectively, whereas there was no change in MAP in the saline group over the same time period. This response was significantly different from the saline treated control animals (p = 0.0051).
In the saline treated group MAP decreased significantly at 1 minute (-16 ± 2%, p = 0.0021) followed by an increase at 10 minutes (+8 ± 2% p = 0.0049) until 20 minutes (p = 0.0100). MAP returned values not different from pre-augmented readings at 30minutes. In the Sildenafil treated group there was no significant change in MAP following bone augmentation. Overall the MAP response in the Sildenafil group was significantly smaller than the saline control group (p = 0.0475). The time to peak response varied between animals and was analysed separately.
Femur pressurisation caused a large transient decrease in MAP (figure 1B open symbols) in both saline (53 ± 3 versus 61 ± 3 mmHg, p = 0.0028) and Sildenafil groups (38 ± 4 versus 58 ± 6 mmHg, p = 0.0013) compared to pre-pressurisation values. There was no difference in the magnitude of the response in the two groups.
Sildenafil (intra peritoneal) had no effect on HR. Furthermore, in the saline group, bone augmentation had no measurable effect on HR. In the Sildenafil group, in response to bone augmentation, HR increased by 3 ± 1% (p = 0.0438) at 1 minute and returned to pre-augmentation values until at 60 minutes when HR increased by 12 ± 4% (p = 0.0316).
Fig. 2 shows typical examples of images of the blood vessels in lungs of control and Sildenafil rats generated using micro CT. We calculated the perfused lung volume from this data and Sildenafil treatment resulted in a 66% (p = 0.0152) greater perfused lung volume (4.7 ± 0.7 cm3 versus 2.8 ± 0.4 cm3). Counting the number of fat emboli in oil Red-O stained lung sections we found no differences in the number of emboli between control (245 ± 74) and Sildenafil treated rats (246 ± 63).
.JPG)
.JPG)
.JPG)
Figure 2. Micro CT images of radiopaque contrast filled blood vessels of control (A) and Sildenafil (B) treated animals following medullary pressurisation.
Discussion
The main outcome of this study is that pre-treatment with the PDE5 inhibitor, Sildenafil, significantly attenuated the increase in PAP resulting from fat emboli generated by bilateral femur cement augmentation in the rat. Sildenafil treatment was associated with a significantly greater perfusion of the lungs. However, this was not associated with an increase in fat emboli escaping into the systemic circulation.
Sildenafil, in male rats, has a relatively short half-life (≈0.3h).[11] Therefore, to ensure a sustained blockade of the PDE5 for the duration of experimental protocol, a dose of 5 mg kg-1 was used. Intra peritoneal injection of Sildenafil caused a decrease in both MAP and PAP, due to a decrease in vascular resistance associated with the increase in nitric oxide. The decrease in MAP was not associated with tachycardia, which is consistent with the observationsof Al-Hessayen et al [12] in heart failure patients, and probably is a consequence of the increase in cardiac sympatheticnerve activity increase due to the fall in MAP being opposed by the decrease in cardiac sympathetic nerve activity as a result of the unloading of the cardiopulmonary baroreceptors.[12]
The vascular response to intramedullary pressurisation of both femurs is presented in Fig. 1. The initial response to pressurisation was a rapid increase in PAP (Fig.1A) and decrease in MAP (Fig.1B). The PAP rise had two components, a large transient doubling of the PAP and recovery, followed by a smaller more prolonged increase in PAP. This was then followed by a sustained increase in PAP and MAP, which persisted for at least 20 minutes. The rapid transient increase in PAP was probably the result of fat emboli entering the pulmonary circulation and creating a mechanical obstruction. This would lead to a transient decrease in venous return to the left side of the heart, a decrease in cardiac output and account for the rapid drop in MAP. These observations are consistent with that observed in a previous study from this research group following vertebroplasty in anaesthetised sheep, which was associated with a rapid transient decrease in cardiac output.[4]
The more sustained pressure effect was probably a result of initiation of a neurogenic reflex pulmonary vasoconstriction,[13] and/or release of vasoconstrictors by activated platelets and leukocytes within the fat emboli. In addition, the endothelial cells of the blood vessels would release vasoactive substances.[13]
Pre-treatment with Sildenafil, while dropping PAP and MAP, had no effect on the peak PAP response to medullary pressurisation, supporting the idea that this response was due to mechanical obstruction. However, the more prolonged increase in PAP, in response to medullary pressurisation, was greatly attenuated by pretreatment with Sildenafil and returned to pre-pressurisation values much more quickly than in the control animals (Fig. 1A). Furthermore, there was no change in MAP in the Sildenafil treated animals following cement pressurisation (Fig. 1B). The effects of Sildenafil in the current study are consistent with those reported in sheep,[14] in which Sildenafil treatment attenuated or abolished the cardiovascular changes associated with vertebroplasty. However, the results between the two studies differ with respect to the distribution of fat within the lung. In the present study, we observed no difference in the number of fat emboli between control and Sildenafil treated rats, whereas, Krebs et al14 reported a 5-fold decrease in the number of fat emboli following Sildenafil treatment which may reflect fat passing through the dilated blood vessels into the systemic circulation. Alternatively, the distribution of fat was much greater in the sheep treated with Sildenafil as a result of dilation of the vasculature, and, by necessity, relatively limited lung samples were taken leading to a sampling error. This idea is supported by the fact that there was no reported fat emboli in the kidneys of the sheep,[14] a typical site for emboli to accumulate. In the current study, the small size of the rat lung permitted a much greater sample of tissue to be analysed.
Using micro CT, it was possible to image the entire lung of the rat, providing good detail of the lung vasculature in the Sildenafil and control animals following pressurisation of both femurs (Fig. 2). Using this novel approach we were able to clearly demonstrate that the lungs from control rats, that had undergone medullary pressurisation, had narrowing of the large pulmonary blood vessels and poor perfusion of the microcirculation (Fig. 2A). In clear contrast, in Sildenafil treated animals micro CT revealed a significantly greater perfusion of the microcirculation (Fig. 2B) and containing the same amount of fat emboli.
Fat emboli, entering the lungs initiate a range of effects, which include mechanical obstruction, neurogenic reflex pulmonary vasoconstriction,[13] release of vasoconstrictors by activated platelets and leukocytes from the fat emboli and endothelial cells of the pulmonary blood vessels.[13]
The presence of mechanical obstruction in the lungs will directly increase the vascular resistance, and in the current study this wasobserved as a relatively transient effect as the bolus of fat entered the pulmonary circulation prior to breaking up and blocking smaller blood vessels. If fat was a non-thrombolytic agent it would require 60–70% of the pulmonary vasculature to be obstructed before there was an increase in PAP.[13] However, because it’s thrombolytic properties a similar increase in PAP can be achieved by 25–30% obstruction of the pulmonary blood vessels. [13] Dias-Junior et al[15, 16] used microspheres (300μm) to create a pulmonary embolism in dogs. They injected sufficient microspheres to increase the PAP by 24 mmHg, which dropped by 42% when Sildenafil was administered.
In conclusion we have demonstrated that the increase in pulmonary pressure resulting from fat emboli entering the circulation is significantly attenuated by the administration of Sildenafil, a phosphodiesterase type 5 inhibitor, without an increase in fat gaining access to the systemic circulation. These findings are of clinical relevance in the prevention of cardiorespiratory complications following surgical procedures generating a large amount of fat emboli as for example fixation of long bone fractures in multitrauma and joint arthroplasty surgery. However further human studies will be required to confirm this.
Acknowledgements
Assistance with the study:We would like to thank Dr Daryl Schwenke for his assistance with this study.
Financial support and sponsorship:Stryker New Zealand Ltd,Mount Wellington. Auckland, New Zealand
Conflicts of interest: none declared
References
- Taviloglu K, Yanar H. Fat embolism syndrome. Surgery Today 2007; 37:5-8.
- Mellor A, Soni N. Fat embolism. Anaesthesia 2001; 56(2): 45-154.
- Aebli N et al. Spine 2002; 27: 460-466.
- Aebli N et al. Pressurization of vertebral bodies during vertebroplasty causes cardiovascular complications: an experimental study in sheep. Spine 2003; 28(14): 1513-1519.
- Aebli N et al. Cardiovascular changes during multiple vertebroplasty with and without vent-hole: an experimental study in sheep. Spine 2003; 28(14): 1504-1511.
- Krebs MO et al. Acute hypoxic pulmonary vasoconstriction in conscious dogs decreases renin and is unaffected by losartan. Journal of Applied Physiology 1999; 86(6): 1914-9.
- Murphy P et al. Relationship of fat embolism to haemodynamic and echocardiographic changes during cemented arthroplasty. Canadian Journal of Anaesthesia 1997; 44(12): 1293-1300.
- Archer S, Michelakis E. Phosphodiesterase type 5 inhibitors for pulmonary arterial hypertension. New England Journal of Medicine 2009; 361(19): 1864-1871.
- Mourani P et al. Effects of long-term sildenafil treatment for pulmonary hypertension in infants with chronic lung disease. Journal of Pediatrics 2009; 154(3): 379-284.
- Yin J et al. Sildenafil preserves lung endothelial function and prevents pulmonary vascular remodeling in a rat model of diastolic heart failure. Circulation Heart Failure 2011; 4(2): 198-206.
- Walker D. Pharmacokinetics and metabolism of sildenafil in mouse, rat, rabbit, dog and man. Xenobiotica 1999; 29(3): 297-310.
- Al-Hesayen A, Floras J, Parker J. The effects of intravenous sildenafil on hemodynamics and cardiac sympathetic activity in chronic human heart failure. European Journal of Heart Failure 2006; 8(8): 864-869.
- Stratmann G, Gregory G. Neurogenic and humoral vasoconstriction in acute pulmonary thromboembolism. Anesthesia and Analgesia 2003; 97(2): 341-354.
- Krebs J et al. Sildenafil prevents cardiovascular changes after bone marrow fat embolization in sheep. Anesthesiology 2007; 107(1): 75-81.
- Dias-Junior C et al. Sildenafil improves the beneficial haemodynamic effects of intravenous nitrite infusion during acute pulmonary embolism. Basic and Clinical Pharmacology and Toxicology 2008; 103(4): 374-379.
- Dias-Junior C et al. Sildenafil selectively inhibits acute pulmonary embolism-induced pulmonary hypertension. Pulmonary Pharmacology and Therapeutics 2008; 18(3): 181-185.





