A Radio-Anatomical Study of Ponticles on Atlas: Clinical point of View
Jyothi S.R1*, Joish Upendra Kumar2, Vinay S.R3
1 Chikkaballapur Institute of Medical Sciences, Chikkaballapura, Karnataka, India
2 SDM College of Medical Sciences & Hospital, Dharward ,Karnataka, India.
3 Doddaballapur General Hospital, Doddaballapur, Karnataka, India.
*Corresponding Author
Dr. Jyothi S.R,
Assistant Professor, Department of Anatomy, India.
E-mail: jyothisr39@gmail.com
Tel: 9739724658
Received: November 27, 2023; Accepted: January 04, 2024; Published: January 19, 2024
Citation: Jyothi S.R, Joish Upendra Kumar, Vinay S.R. A Radio-Anatomical Study of Ponticles on Atlas: Clinical point of View. Int J Anat Appl Physiol. 2024;10(1):223-227.
Copyright: Jyothi S.R@2024. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Atlas, an atypical 1st cervical vertebra with anterior and posterior arch supports the globe of the head. The atlas,
shows extensive variability in its morphology. Sometimes bony outgrowths known as ponticle (bridge) extend from lateral
mass to the posterior arch of atlas or to the posterior root of transverse process, which may be complete or incomplete and,
can compress the vertebral artery during its course from foramen transversarium to foramen magnum of skull.
Aims: Observefor different type of ponticles on dry bone, as well as on CT scans of individuals. To aid the clinicians in diagnosing
vertebrobasilar insufficiency & surgeons during screw fixation.
Materials & Methods: Cross sectional descriptive study was carried out involving 100 CT scans and60 dried macerated 1st
cervical vertebrae. Individuals found to have fractures, lesions, dislocations of atlas, on CT scan images, were excluded from
the study. All dried vertebrae were intact and free from osteophytes.
Sampling method: Convenience non- probability sampling method.
Results: Dry bone specimens presented with, complete ponticulus posterior in 5% specimens, and incomplete ring in 30%,
complete ponticulus lateralisin 1.6% specimen and incomplete ponticulus lateralis in 3.3% specimens,retrotransverse foramenin
3.3% of specimens. CT scan depicted - Type B variety of posterior ponticle in 6 females & 9 males, Type C in 2 females
& 4 males &Type D in 1 male individual. Retrotransverse foramen was seen in 2 male individuals.
Conclusion: The present study is of importance to orthopaedicians, neurosurgeons during spinal surgeries especially during
transarticular and transpedicular screw fixation. It also aids otorhinolaryngologist while handling patients with symptoms of
vertebrobasilar insufficiency.
2.Introduction
3.Conclusion
4.References
Keywords
Atlas Vertebra; Ponticulus Posterior; Ponticulus Lateralis; Retroarticular Canal; Retrotransverse Foramen.
Introduction
The atlas, the first cervical vertebra is named after �ATLAS� who
according to Greek mythology supported the Earth on his shoulders.[
1] The atlas holds the globe of the head and is unique in that
it fails to incorporate a centrum, whose position is occupied by
dens of axis. The atlas consists of two lateral masses connected
by a short anterior arch and a longer posterior arch. The laminae
and pedicles form the posterior arch, which contributes to threefifths
of the circumference of the atlantal ring. The superior surface
of posterior arch bears a wide groove for the vertebral artery
and venous plexus immediately behind, and, the dorsal ramus of
first cervical nerve (suboccipital nerve) intervenes between them.
The superior and inferior articular facets lie on the lateral masses,
anterior to first and second cervical nerve respectively. The superior
articular facets are concave, kidney shaped and is superomedial.
They receive the condyles of the occipital bone to form an
atlanto-occipital joint which are involved in nodding movements.
The inferior is almost circular, slightly concave, and faces downwards
and medially. The spine is replaced by posterior tubercle. [2,
3] The superior border of posterior arch gives attachment to the
posterior atlanto occipital membrane. The third part of vertebral
artery courses from foramen transversarium of the atlas towards
the groove on the posterior arch of atlas and then runs upwards
into cranial cavity to form basilar artery. The vertebral artery is
predisposed to damage by any bony or ligamentous structures
during this course. Sometimes a bony outgrowth known as ponticle
(bridge) flanges over the groove either in posterior/lateral/posterolateral position. The bony spur extending from dorsal side
of lateral mass to the posteriormargin of the groove is posterior
ponticle, which could be partial or complete. When complete, it
describes a foramen known as �Retroarticularcanal� (RAC) or arcuate
foramen, if partial then forms ponticulus posticus or Kimmerley
anomaly. The bony outgrowth from lateral margin of the
lateral mass to the posterior root of transverse process is the lateral
ponticle. It may present as partial or complete form. When
complete it forms supratransverse foramenor lateral vertebral foramen.
The posterolateral ponticle is a bony fragment from the
lateral margin of posterior 1/3rd of lateral mass to transverse
process and dorsal edge of posterior arch of atlas.[4] Individuals
with retroarticular canal may present with vertebrobasilarinsufficiency
presenting with dizziness, fainting and transient diplopia
during extreme rotation of neck.[5] During flexion and extension
of the neck, the bony foramen may limit the normal mobility of
the vessels and may cause disturbances of arterial flow and of
the periarterial sympathetic plexus giving rise to the symptoms of
vertebrobasilar insufficiency syndrome. The vertebral artery can
get pinched off during neck rotations leading to thrombosis and
embolism, which may lead to cerebellar infarction. Ossification
of ligamentous structures is very frequently observed in various
parts of the body, which may result in compression of neighboring
structures and complications in regional surgeries.[6] The
instability of atlantoaxial complex or occipitocervical junction
caused by traumatic or nontraumatic conditions are corrected by
surgical techniques such as interlaminar clamp, interspinous wiring,
plate and screw fixation and very recently, trans articular and
transpedicular screw fixation have been used to stabilize the cervical
column.Improper insertion of pedicle screw can damage vital
structures such as spinal cord, nerve roots,cranial nerves and vertebral
arteries.[7] Surgeons operating at craniovertebral junction
should be aware of different variations of this three-dimensional
structure, the atlas vertebra. Physicians and neurologists should
think of bony spur from lateral mass of atlas as predisposing factor
for vertebrobasilar insufficiency. The main objective of this
study was to look for presence of ponticles, its type both in dry
bones and in CT scan.
Materials and Methods
Cross-sectional descriptive study was undertaken in a tertiary care
center between January to April 2021, wherein, 100 consecutive
CT scans of adults done in study period, in which occipito-cervical
regions were included in the scans and 60 dry and fully ossified
adult human atlas vertebrae, which were available in the Anatomy
Department, were included. Institutional Ethical clearance was
obtained prior to the study [KVGMC&H/SUL/IEC/39/OCT
2022]. A 128 slice Siemens CT scanner was used for obtaining CT
images. Images of 1mm thickness were reconstructed from the
raw dataset in bone windowing and viewed in all three planes in
multi-planar reformatting algorithm. Informed consent of individuals
who underwent CT scans was obtained prior to including
their imaging dataset into the study. Each type of ponticle was
meticulously documented by experienced Radiologist according
to classification based on Parita K et al [8]. An Anatomist studied
the detailed anatomy of dry atlas vertebrae,its features � arches,
surfaces, lateral mass & its transverse process referring to Cunningham�s
manual [3] and recorded various type of ponticles.
Inclusion criteria: adult subjects who underwent a cervical CT
examination in which the C1 vertebra could clearly be seen and
who did not present traumatic fractures involving the cervical
spine. Please note the clinical indications for the CT examination
for each CT scan Sample: cerebral ischemic stroke, for syncope,
for headache, for another neurological symptomatology (tinnitus,
amaurosis fugax, diplopia, etc.) and for other causes including, but
not restricted to, preoperative cardiac surgery, subarachnoid hemorrhage
and drop attack. All samples of atlas were inspected to
ensure that the vertebrae were intact and free from osteophytes.It
was observed carefully for the different ponticuli from the lateral
mass. The variations were noted and photographed.
Exclusion criteria: fractures, degenerative diseases of the cervical
spine, cervical spine fracture/dislocation, rheumatoid arthritis,
previous history of surgery, tumors, or cervical myelopathy with
a spinal canal diameter of =12 mm.
Sampling method: Convenience non- probability sampling method
Statistical analysis: Data was entered in an Excel sheet & SPSS
version 26 was used for statistical analysis. Qualitative data was
expressed in the form of frequency & percentage. Chi-square test
was used to find out association between the 2 variables. Quantitative
data, age of the patient was expressed in the form of mean.
Results
Dry bone specimens were observed for different ponticuli & recorded.
Retroarticular canal (Complete ponticulus posterior) in 3
(5%) specimens, and incomplete ring in 18 (30%) specimens was
observed. Supratransverse foramen (Complete Ponticulus lateralis)
was seen in 1 (1.6%) specimen and incomplete ponticulus
lateralis in 2 (3.3%) specimens. Retrotransverse foramen was seen
in 2(3.3%) of specimens. (Table 1,2,3 & 4)(Figure 1).
The mean age of participants underwent CT scans was 31.4 years
and included 43 females and 57 males. Type B variety of posterior
ponticle was seen in 6 females & 9 males(chi square = 0.277, p
value = 0.87), Type C was seen in 2 females & 4 males(chi square
=1.5, p value= 0.47). Type D (complete posterior ponticle � Retroarticular
canal) in 1 male individual (chi square not applicable),
(Figure2) & (Table 5). Retrotransverse foramen was seen in 2 male individuals. The comparison b/w sex & sides were not statistically
significant.
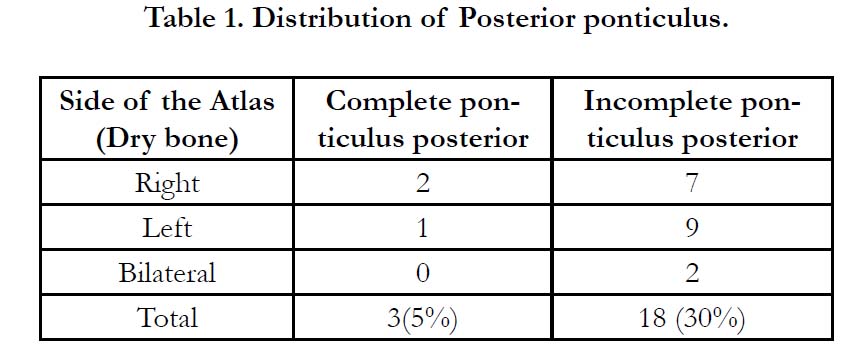

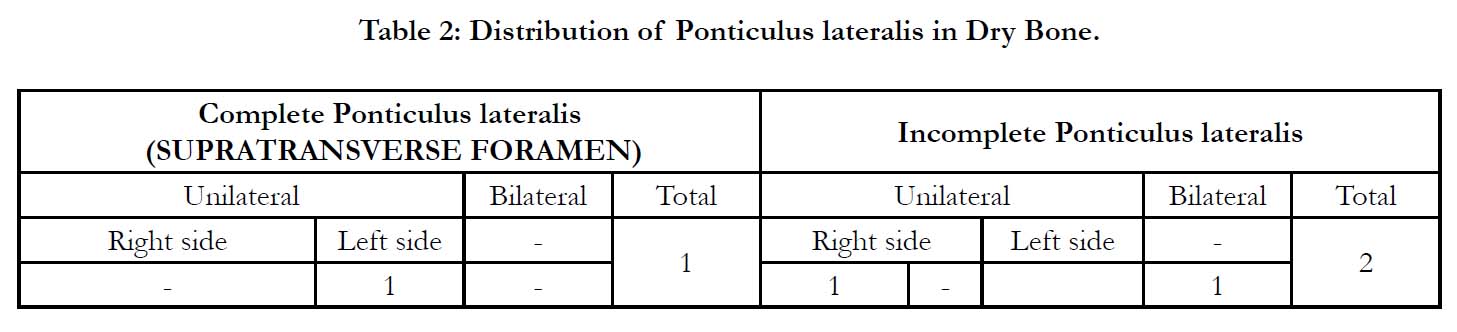
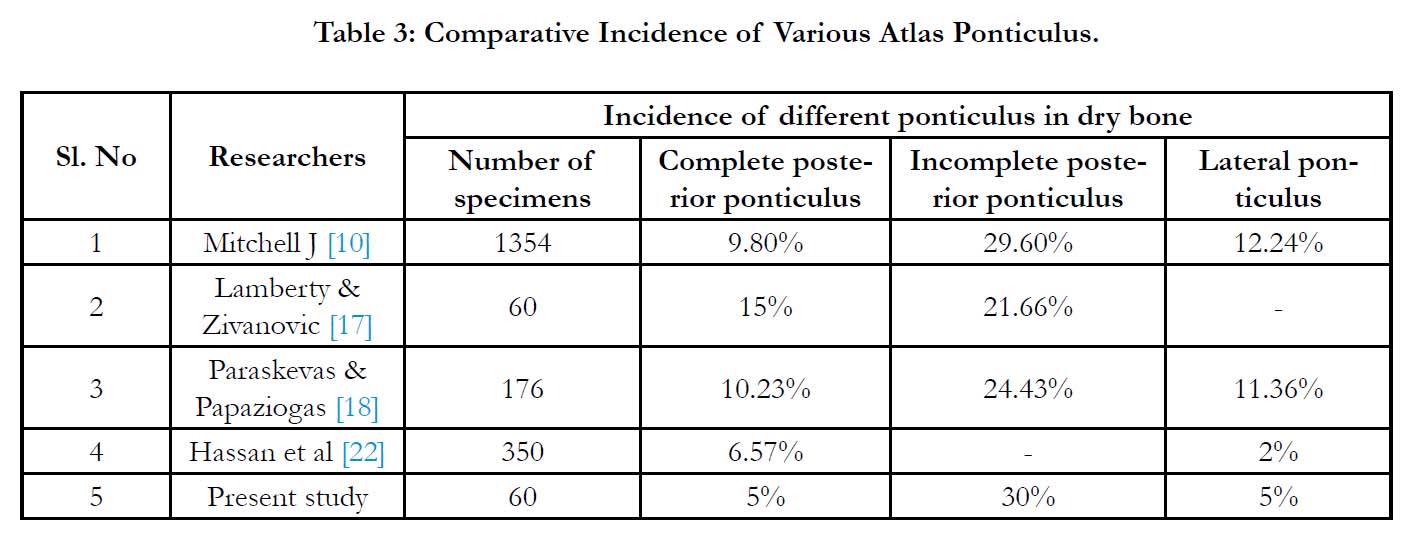
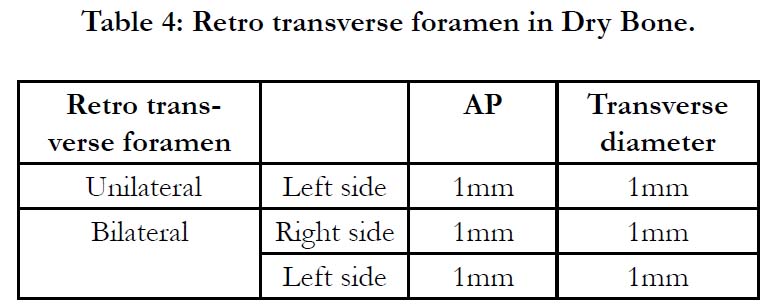
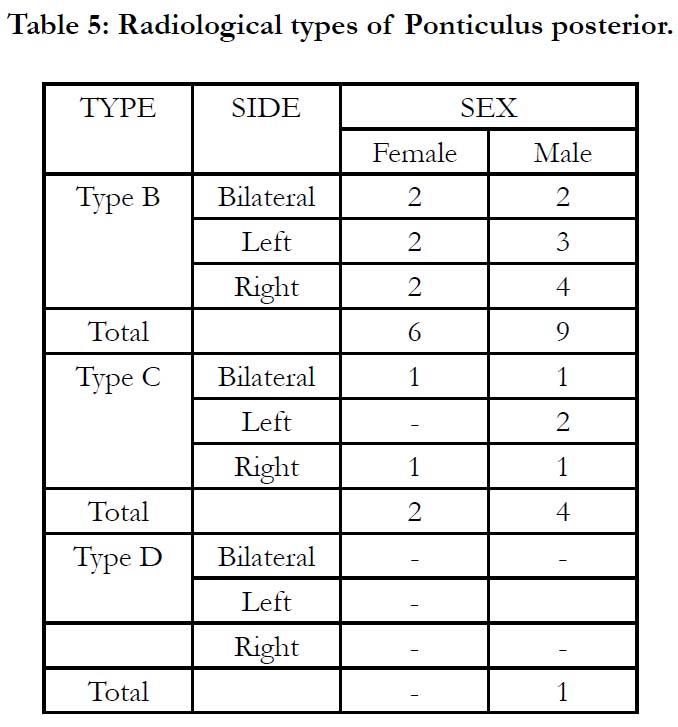
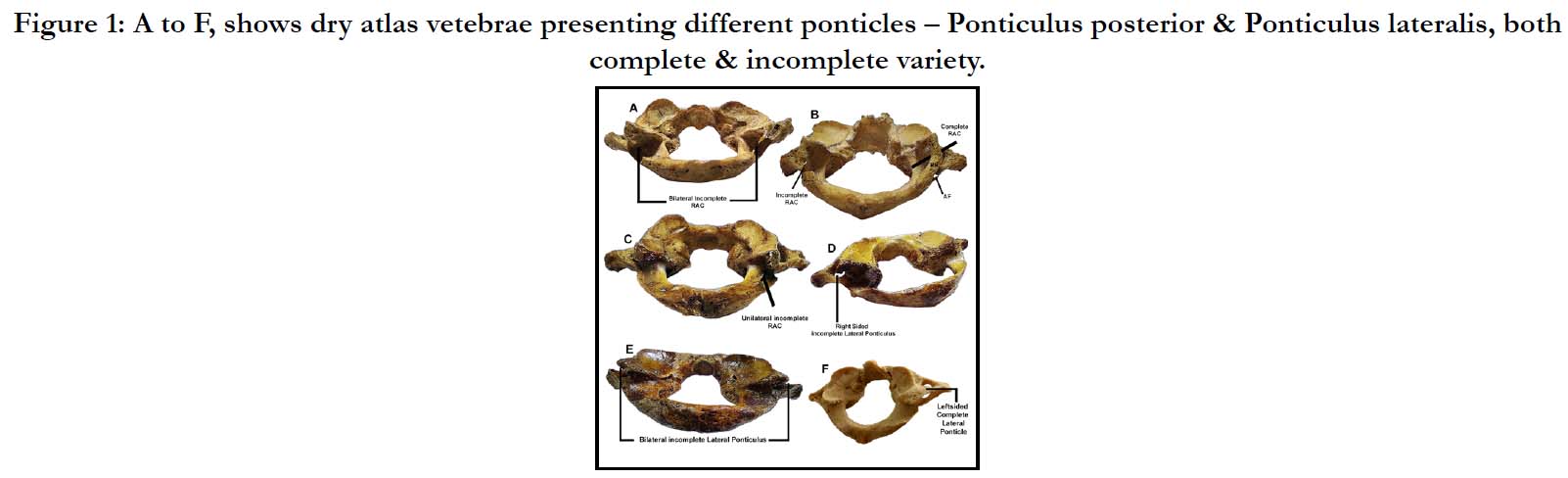

Figure 1: A to F, shows dry atlas vetebrae presenting different ponticles � Ponticulus posterior & Ponticulus lateralis, both complete & incomplete variety.
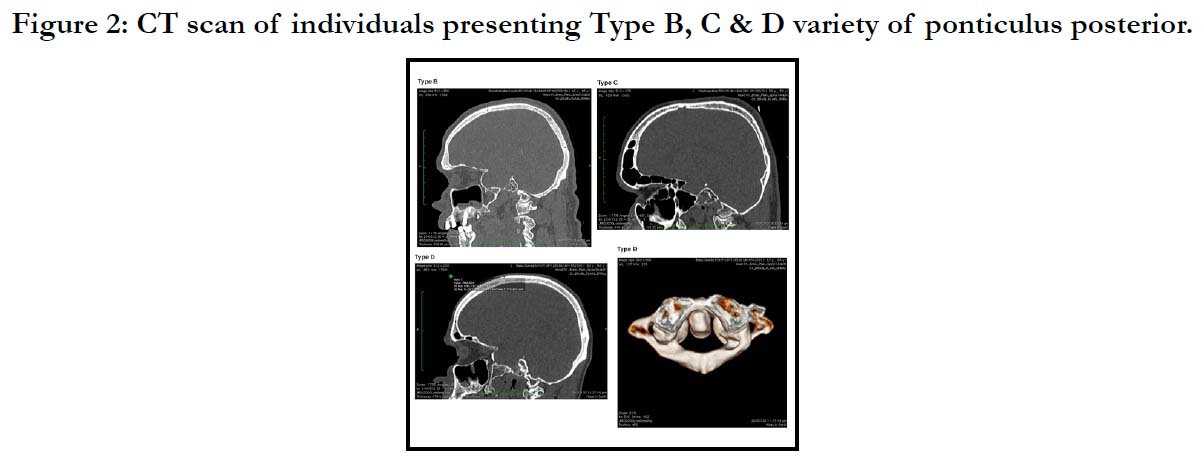

Figure 2: CT scan of individuals presenting Type B, C & D variety of ponticulus posterior.
Discussion
Recently various surgical techniques and instrumentation have
been employed to stabilize the unsteady cervical spine. The management
of various traumatic, congenital or neoplastic conditions
associated with atlas and its joints require more information about
the bone and its adjacent anatomy. The knowledge on different
ponticles of atlas vertebra may be helpful to overcome complications
such as vertebral artery injury, spinal cord injury and cranial
nerve damage during C1 stabilizing operation and in diagnosis of
vertebrobasilar insufficiency syndrome. [9, 10]
Among all cervical vertebrae the atlas is known for its variations.
The atlas ponticle are shared structure between human and nonhuman
primates. [11, 12]
Parita K et al [8] describes radiological classification of posterior
ponticle in detail as below and the results obtained in our study is
depicted in (Table 5).
Type A: Normal - No degree of this anomaly can be detected;
including exaggerated grooving of the fossa arterialis with no distinct
spicule.
Type B: Trivial - Partly developed foramen ranging from a minute
but distinct spicule to a developing bridge that encases less than
50% of the circumference of the vertebral artery.
Type C: Partial, well-developed -Well-developed foramen encases
at least the majority (greater than 50%) of the vertebral artery�s
circumference.
Type D: Complete - The vertebral artery is completely encased
by bone
Bipedalism and acquisition of erect posture might have led to
the regressive and disappearing phenomenon in atlas leading to
formation ofponticles. [13] Macalister was the first to report the
posterior and lateral ponticles. Number of theories has been postulated
to explain the ponticles.One theory explains that it is due
to persistence of superior oblique process of other mammals.[14]
According to some authors it develops from dorsal arch of proatlas
and belongs to occipital vertebra.[15] Le Double described
that ponticles could be due to ossification of the lateral fibers
of posterior atlanto-occipital membrane or acquired ossification
of oblique ligament, due to pulsation of vertebral artery [13] or
by external mechanical factor like carrying heavy objects on the
head.[16] Some authors have postulated that the lateral extension
of proatlas may lead to the formation of lateral ponticles. [17]
Lamberty and Zivanovic observed the bony ring in atlas of two
children�s skeleton aged 2 and 4 years and also in the cervical spine
x-ray of a 13-year-old boy. From this observation they inferred
that ossification of a ligament does not occur normally in such
young persons.[18] Paraskevas G et alexplained that incomplete
bony ponticuli are precursor of the complete bony ponticuli.
[19] The same was also observed by Kendrick GA and Biggs NL
where in, they found in two females unilateral incomplete posterior
ponticle changed to complete ring over duration of 1to 2
years.[20]
The procedures like atlas screw fixation have gained popularity to
such an extent that it has increased the need for thorough evaluation
of the anatomy of C1 vertebra and the vertebral artery. During
the above procedures if any injury to vertebral artery may lead
to severe intraoperative bleeding and may cause unpredictable
neurological deficits, depending on the adequacy of blood flow
from the contralateral vertebral artery.[21] When patients present
with symptoms like pain in temporal region, pain in back of eye,
vertigo and paresthesia of hand radiography of cervical spine is
the simplest and useful aid to detect the presence of ponticles.
[22] Hassan M et al classified posterior bridges into 6 classes [23].
Class 1 - included those having only the impression of vertebral
artery on the posterior arch of atlas
Class 2 - included those having deeper impression like groove or
sulcus for the vertebral artery
Class 3 � included those in which partial ponticulus posterior was
present as a bony spicule.
Class 4- included those having complete ponticulus posterior
Class 5 � included those having ponticulus lateralis which extended
from the lateral mass to the transverse process
Class 6 � included those having postero- lateral tunnel i.e., combination
of complete ponticulus posterior and ponticulus lateralis.
In the present study, type class 2 was seen in 14(23.3%) of specimens,
type class 3 was seen in 18(30%) of specimens, type class 4
was observed in 3(5%) of specimens and type class 5 was seen in
3(5%) of specimens.
Satheesha Nayak reported retro transverse foramen in one specimen
and right being larger than left.[24] In the present study, we
observed in one specimen on left side among the dry bone of
atlas. CT scan of atlas showed such retrotransverse foramen in
two cases.
Conclusion
Extreme rotation of head and neck may compress vertebral artery.
This may get aggravated by presence of retroarticular canal
for vertebral artery, resulting in stenosis and compromised blood
flow.Hence the present anatomical study was undertaken to study
the differentponticles of atlas vertebra. The awareness may be
helpful to neurosurgeons and orthopaedicians while approaching
craniocervical junction through posterior route. The detail knowledge,
also aids neurophysicians and otolaryngologists to treat patients
presenting with symptoms of vertebrobasilar insufficiency.
To achieve optimal therapeutic results, a complete understanding
of the morphology is indispensable.
Conflicts of Interests: None
Acknowledgements
The authors sincerely thank those who donated their bodies to
science so that anatomical research could be performed. Results
from such research can potentially increase mankind�s overall
knowledge which can then improve patient care. Therefore, these
donors & their families deserve our highest gratitude.[25]
References
- [1]. MooreKL. Clinical Oriented Anatomy.The back.3rd ed.Baltimore:Williams and Wilkins; 1992:331
- Standring S. Gray�s Anatomy.The anatomical basis of clinical practice. The back. 40thed.Philadelphia: New Elsevier Churchill Livingstone; 2008 :719 .
- Romanes G J. Cunningham�s manual of practical anatomy. The head and neck. 15th ed. Oxford: Oxford Medical Publications;2006;3:2
- Patel NP, Gupta DS, Parmar ND. Incidence of ponticles in human atlas vertebrae: a study from South Gujarat population. Indian J Clin Anat Physiol. 2015;2(3):135-9.
- Sylvia S, Kulkarni S, Hatti A. Bilateral retro articular ring in atlas vertebra a case report. Anatomica Karnataka. 2011;5(1):81-6.
- Cakmak O, Gurdal E, Ekinci G, Yildiz E, Cavdar S. Arcuate foramen and its clinical significance. Saudi Med J. 2005 Sep 1;26(9): 447-451.
- SENG�L G, KADIOGLU HH. Morphometric anatomy of the atlas and axis vertebrae. Turk. Neurosurg. 2006;16(2):69-76. https://scholar.google. com/scholar?hl=en&as_sdt=0%2C5&q=Morphometric+anatomy+of+the+a tlas+and+axis+vertebrae&btnG=
- Chitroda PK, Katti G, Baba IA, Najmudin M, Ghali SR, Kalmath B, et al. Ponticulus posticus on the posterior arch of atlas, prevalence analysis in symptomatic and asymptomatic patients of gulbarga population. J Clin Diagn Res. 2013 Dec;7(12):3044-7.Pubmed PMID: 24551723.
- Gupta C,Radhakrishnan P, Palimar V, D�Souza AS, Kiruba NL. A quantitative analysis of atlasvertebrae and its abnormalities. J. Morphol. Sci 2013;30(2):77-81
- Lalit M, Piplani S, Kullar JS, Arora AK, Mannan R. The morphological analysis of the superior articular facet of the adult human atlas vertebra. J Clin Diagn Res. 2011 Apr;5(2):274-77.
- Mitchell J. The incidence and dimensions of the retroarticular canal of the atlas vertebra. Acta Anat (Basel). 1998;163(2):113-20. Pubmed PMID: 9873140.
- MITCHELL J. The incidence of the lateral bridge of the atlas vertebra. J Anat. 1998 Aug;193(2):283-5.
- Lalit M, Piplani S, Arora AK, Kullar JS, Sharma T. Incidence of atlas bridges and tunnels: Their phylogeny, ontogeny and clinical implications. Rev Arg de Anat Clin 2014;6(1)26-34
- Macalister A. Notes on the homologics and comparative anatomy of the atlas and axis. J Anat and Physiol 1869;3:54-64.
- Von Torklus D, Gele W. The upper cervical spine. New York: Grunne and Stratton;1972:28-30.
- Taitz C, Nathan H. Some observations on the posterior and lateral bridge of the atlas. Acta Anat(Basel). 1986 Jul 15;127(3):212-7.
- Allen W. The Varieties of the Atlas in the Human Subject, and the Homologies of its Transverse Processes. J Anat Physiol. 1879 Oct;14(Pt 1):18-28. Pubmed PMID: 17231305.
- Lamberty BG, Zivanovic S. The retro-articular vertebral artery ring of the atlas and its significance. Acta Anat (Basel). 1973;85(1):113-22.Pubmed PMID: 4197316.
- Paraskevas G, Papaziogas B, Tsonidis C, Kapetanos G. Gross morphology of the bridges over the vertebral artery groove on the atlas. Surg Radiol Anat. 2005 Apr;27(2):129-36.Pubmed PMID: 15800734.
- KENDRICK GS, BIGGS NL. Incidence of the ponticulus posticus of the first cervical vertebra between ages six to seventeen. Anat Rec. 1963 Mar;145:449-51.Pubmed PMID: 14031912.
- Simsek S, Yigitkanli K, Comert A, Acar HI, Seckin H, Er U, et al. Posterior osseous bridging of C1. J. Clin. Neurosci. 2008 Jun 1;15(6):686-8.
- Parkin PJ, Wallis WE, Wilson JL. Vertebral artery occlusion following manipulation of the neck. N Z Med. 1978 Dec 1;88(625):441-3.
- Hassan M, Sulka S, Siddiqui MS, Singh D.Posterolateral tunnels and ponticuli in human atlas vertebrae. J Anat2001;199:339-343
- N Satheesha, V Venkata Ramana and R Deepthinath. Neuroanatomy 2005; 4:39
- Iwanaga J, Singh V, Ohtsuka A, Hwang Y, Kim HJ, Morys J, et al. Acknowledging the use of human cadaveric tissues in research papers: Recommendations from anatomical journal editors. Clin Anat. 2021 Jan;34(1):2-4. Pubmed PMID: 32808702.





