Lower Extremities Biomechanics Patterns of Obese and Normal Body Mass Adults during Stairs Ascent and Descent
Egret C*, Ransom A, Amasay T, Ludwig K
College of Nursing and Health Sciences, Sport and Exercise Sciences Program, Barry University, Miami Shores, Florida, USA.
*Corresponding Author
Claire Egret, PhD,
College of Nursing and Health Sciences, Sport and Exercise Sciences Program,
Barry University, Miami Shores, Florida, USA.
Tel: (305) 899-3064
Fax: (305) 899-4809
E-mail: cegret@barry.edu
Received: October 11, 2019; Accepted: October 25, 2019; Published: October 28, 2019
Citation: Egret C, Ransom A, Amasay T, Ludwig K. Lower Extremities Biomechanics Patterns of Obese and Normal Body Mass Adults during Stairs Ascent and Descent. Int J Anat Appl Physiol. 2019;5(4):119-123. doi: dx.doi.org/10.19070/2572-7451-1900022
Copyright: Egret C©2019. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Obesity has been found to be associated with functional and structural limitations, which included differences in normal gait, and in ascending and descending stairs. The purpose of this study was to investigate the differences between ascending and descending stairs in an obese population compared to a normal body mass (normal mass) population. Eleven obese (BMI 34.5+0.92 kg/m2) and 13 normal mass (BMI 23.39+0.36 kg/m2) adults participated in this study. Lower extremity kinematic and kinetic data were collected while ascending and descending the stairs at self-selected walking speeds. A repeated measures ANOVA identified significant differences between the obese and normal mass groups. Normal mass group had a significant higher range of motion (ROM) at hip and knee flexion/extension ROM (p < 0.05), and at ankle inversion/eversion ROM (p < 0.001) during stair descending, and higher knee flexion/extension ROM (p < 0.05) during stair ascending. The normal mass group had a higher peak hip adduction and peak knee abduction moments (p < 0.05) during stair descending. On the other hand, the obese group had a higher peak hip adduction moment and peak knee anterior shear force (p < 0.05) during stair ascending. No further differences where observed between the groups. The findings indicate that obese individuals adopt a different kinematic and kinetic stair ascending and descending strategies. The strategies adopted by the obese group may be an attempt to better dissipate the larger ground reaction forces due to their increased weight.
2.Introduction
3.Methods
3.1 Participants
3.2 Data Collection
3.3 Procedures
3.4 Data Analysis
4.Results
5.Discussion
6.Conclusion
7.References
Keywords
Obesity; Body Mass Index; Stair Walking.
Introduction
Obesity has been clinically implicated with musculoskeletal disorders such as osteoarthritis (OA) as a result of the direct load involving weight bearing joints [18]. Obesity is the number one risk factor for the progression of knee OA and may have long-term adverse effects on the knee joint [9]. The most prominent physical characteristic seen in knee osteoarthritis is joint space narrowing in the medial and lateral tibio-femoral compartments [1]. Sturmer et al., (2000) [18] reported a strong association between obesity and bilateral knee osteoarthritis which may potentially lead to changes in stair ambulation patterns in an obese population. When the joints of the lower extremity have an added load placed on them, joint degeneration occurs. Gait analyses of obese individuals have identified kinematic and kinetic adaptations when compared to normal body mass (normal mass) population [12], however limited research is available when comparing obese individuals to normal mass individuals during ascending and descending stairs.
Walking, or more specifically gait, consists of an adaptive cycle of balance and lower limb movement [10]. Walking is a very different activity for someone who is obese then for a normal mass individual [10]. One of the earliest indications of impaired gait is a decrease in walking velocity. Several studies have found overweight and obese individuals to have a lower preferred walking speed [7, 8, 12]. The general stride characteristics were significantly different between obese participants walking at self-selected and standard speeds compared to normal mass individuals [8]. Obese participants walked at a 16% slower velocity with a 7% shorter step length, and an 11% lower step rate at the self-selected speed [8]. When the obese group and normal mass group walked at the same velocity the obese participants had a 5% shorter relative swing phase and a 3% longer relative stance phase compared to the normal mass participants [8]. Obese individuals compensated for the excessive body weight by decreasing knee flexion when walking, which led to reducing the forces placed on the knee [15]. Lai et al., (2008) [12], found that during gait obese adults tend to spend more time in the stance phase, which increased their stability [12]. When stability increased, hip and knee adduction angles and ankle eversion angle were higher in the obese group than the normal mass group, during the pre-swing phase. Moreover, ankle plantarflexor moment decreased in the obese group at late stance [12]. The study done by Carvalho et al., (2012) [5] identified that obese participants experienced a greater difficulty in adapting to speeds of walking, outside the normal speed, and that the gait cycle had a greater stance phase and asymmetries in the lower limb. Kinematic modifications included obese adults walking with a shorter step length and an increased in-step width, in order to adapt and keep similar velocities of normal mass adults while walking [15].
Deveita & Hortobágyi (2003) [8] found that obese individuals adopt a more erect posture, smaller knee flexion and a greater ankle flexion, when compared to normal mass individuals. Browing & Kram (2007) [4] also measured peak vertical ground reaction force (GRF) values to be approximately 60% greater for obese versus normal mass individuals. Walking slower reduced the ground reaction forces and net muscle moments in obese people [19].
During level walking, obese adults employ a gait strategy of using less knee flexion during stance [4]. However, during ascending and descending stairs obese adults cannot decrease knee flexion thus making the individuals work harder or change the gait pattern, to ascend or descend stairs. Therefore, the obese population may use other adaptations to assist them in ascending and descending stairs. Adaptations may potentially lead to a lower level of mobility and even lower quality of life, in this population. Normal mass healthy individuals generally use a step-over-step (SOS) technique to ascend and descend stairs [16, 17, 20]. Obese individuals typically adopt alternative gait patterns such as the step-by-step (SBS) method (placing both feet on the same step before ascending or descending), walking sideways, or relying on the handrails for stability [11, 17, 20]. Stair ambulation requires a significant amount of balance to stabilize the body during a forward and vertical movement, concentrically and eccentrically, contracting muscles of the lower extremity in order to ascend and descend efficiently [11]. Stair walking is much more demanding than level walking [16]. The difficulty with stair climbing is attributable to increased muscular demands, which are reflected in larger forces [6], angles [2], powers [13], moments [6, 13], and ranges of motion (ROM) [14]. These increased demands occur consistently at the knee joint. Strutzenberger et al., (2011) [17], designed a staircase to study the effects of obesity on the biomechanics of stair-walking in children. They hypothesized that during stair-walking lower extremity joint moments, normalized to body mass,will be greater in obese children than in normal mass children. The obese group had greater hip abduction moments and knee extension moments in the obese group during stair ascent. During stair descent smaller hip extension moments, greater hip flexion moments, and greater knee extension moments were found in the obese group.
Limited research has been conducted on activities of daily living (ADL) such as ascending and descending a flight of stairs in the obese population. The purpose of this study was to investigate the differences between ascending and descending stairs inan obese population compared to a normal mass population. It was hypothesized that the obese group would have a decrease in range of motion at the hip, knee, and ankle, while demonstrating an increase in moments at the hip and knee joints, when compared to the normal mass group.
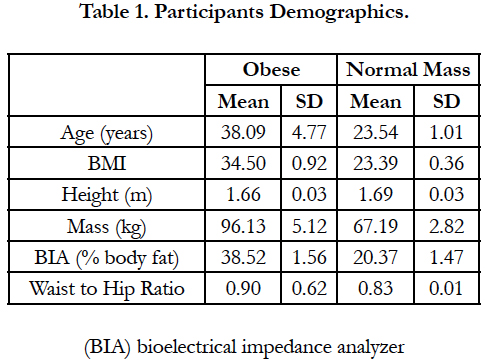
Twenty-four volunteers participated in the study. Participants were broken down into two groups according to BMI. Eleven participants with a BMI over 30 kg/m2 composed the obese group and thirteen participants with a BMI under 25 kg/m2 were considered the normal mass group. The demographic data of all participants are presented in Table 1. Participants were excluded from this study if they experienced a significant change in weight from surgery or any weight loss program, in the six months prior to this study. All participants were clear of any health problems that may compromise their participation. All participants completed a short PAR-Q & You Questionnaire and verbally indicated that they had no current orthopedic abnormalities or any kind of lower extremity joint pain, at the time of testing, that may hinder them from participation in the study. The study was approved by the University Institutional review Board.

Kinematic and kinetic variables were collected using synchronized biomechanical instrumentations. Kinematic variables were collected using seven cameras high speed motion capture system (Vicon Nexus 1.8.1, Centennial, Colorado) at a sampling rate of 240Hz. Sixteen retroreflective markers were placed, according to the plug-in gait model,on the right and left side of the body, along the lower extremity at the posterior superior iliac spine, anterior superior iliac spine, lateral aspect of the femur, the knee at the joint line, lower shank, lateral malleolus, heel, and distal head of the second metatarsals. Kinematic data were filtered using a Woltring quintic spline filter with a cutoff frequency of 20 Hz and analyzed using Polygon 3.1. Kinetic variables were collected using an AMTI force plate (Advanced Medical Technologies, Inc., Watertown, MA) sampled at 960 Hz. All forces and joint moments were normalized to the participant’s body mass.
Body composition was measured with a hand-held bioelectrical impedance analyzer (BIA) (Omron Healthcare, Vernon Hills, IL) at a fixed signal frequency of 50 kHz. Two trials within 1% body fat were obtained for each participant. The average of these two trials was taken for body fat percentage. Waist and hip circumferences were also measured using a standard Gulick tape and evaluated to the nearest 0.1cm.
All data were collected in a single session for each participant. Participants did not warm up before testing procedures to simulate activities that are performed on a daily basis. All participants were asked to wear fitted shorts and shirt and were tested barefoot for each test. Height and mass measurements were taken before testing. These measurements were also taken for the calculation of BMI. All retroreflective markers were secured properly with double sided tape according to plug-in gait placement described above.
For the stair ambulation, participants were given as many practice trials as needed to become familiar with the movement. The experimental staircase was a set of three podium stairs with two handrails positioned 10 cm from the force plates (Figure 1). The step dimensions were rise of 20.5 cm, width across the stair was 31 cm and length of the stairs was 92 cm. No handrail was used when ascending or descending stairs but was present for safety. The force plates were positioned as the first step when ascending the stairs and as the last step when descending the stairs on the floor. Three successful trials at selected speeds were recorded for each participant. Participants were given one-minute rest between trials.


Each participant’s height in meters and mass in kilograms were recorded. This information was used to calculate Body Mass Index (BMI) in kg/m2. The independent variable in the study was body composition category, as determined by BMI (normal mass and obese). The dependent variables included hip and knee flexion/ extension ROM, ankle inversion/eversion ROM, peak ankle inversion moment, peak hip adduction moment, peak knee abduction moment, shear force at the knee, step length, step width, and double and single support time from foot strike to toe off. Ground reaction forces and joint moments were normalized to body mass. A 2X2 repeated measures ANOVA was conducted comparing dependent variables between groups (obese and normal mass) while ascending and descending the stairs.
Results
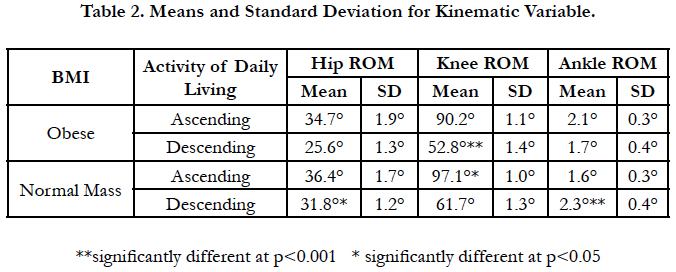
Significant differences in kinematic variables were observed between the obese and normal mass group. Normal mass group had a significant higher hip flexion/extension ROM (p < 0.05), a significant higher knee flexion/extension ROM (p < 0.001), and a significant higher ankle inversion/eversion ROM (p < 0.001) than the obese group, during stair descending. Normal mass group had a significant higher knee flexion/extension ROM (p < 0.05) than the obese group during stair ascending. No other significant differences were observed (Table 2).
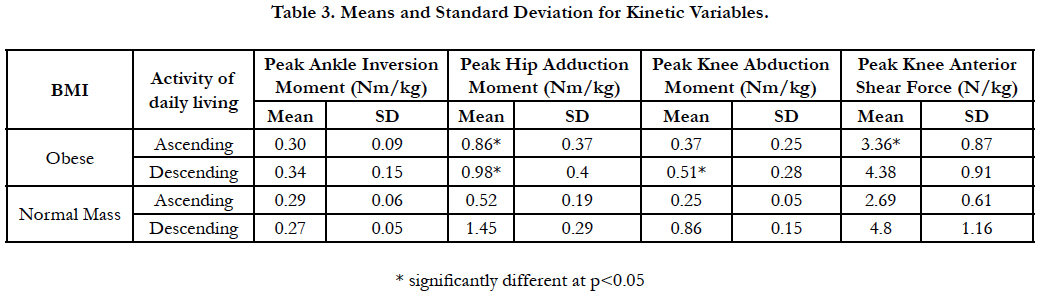
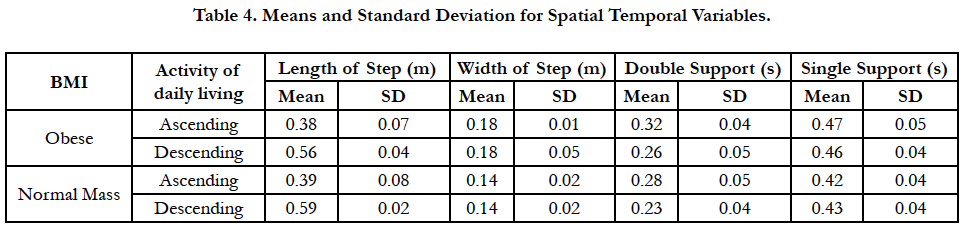
Significant differences in the kinetic variables were observed between the obese and normal mass group. The normal mass group had a higher peak hip adduction moment (p < 0.05) and a higher peak knee abduction moment (p < 0.05) than the obese group, during stair descending. The obese group had a higher peak hip adduction moment (p < 0.05) and a higher peak knee anterior shear force (p < 0.05) than the normal group, during stair ascending (Table 3). No further differences where observed between the groups including for the spatial temporal variables (Table 4).
Discussion
The purpose of this study was to investigate the relation between body mass index (BMI) and lower extremity function of obese and normal mass participants, using an experimental staircase. Kinematic and kinetic variables were compared between obese and normal mass participants during stairs ascending and descending, at self-selected speeds. The first hypothesis stated that there would be significant decrease in the range of motion at the hip, knee, and ankle between obese and normal mass individuals, within each functional test (stair ascending and descending). Our hypothesis was partially supported. Ankle inversion ROM was significantly lower during stair descending in the obese group by 0.6°. Similar results were identified at the knee and hip during stair descending. The obese group had significantly lower knee flexion ROM than the normal mass group by 9°. The hip flexion ROM was smaller in the obese group by 6° than the normal mass group. During ascending, the only significant difference was observed at the knee. The obese group had a smaller knee flexion ROM than the normal mass group by 7°. No significant differences were observed in the ankle and hip during stair ascending. This difference, although not large, may be due to the added mass of the obese group. This is expected as increased body mass usually leads to a reduced range of motion at a joint. This decreased range of motion may be a result of swelling and stiffness accumulating overtime in the joints due to the excessive body mass seen in the obese group. Another aspect can be related to the body position over the base of support. The excessive body mass may cause the obese individual to minimize the movement of the center of gravity out of the base of support to keep their balance, by keeping their body erect.
Average walking velocity is typically 1.2m/s for obese individuals and 1.4m/s for normal mass individuals [8]. As an individual gain more mass, become more obese, their walking velocity seems to decrease. In 2003, DeVeita and Hortobagyi found that the obese population walked at a 16% slower velocity than the normal mass population, which was related to the 7% decrease in step length and the 11% lower step rate, at their self-selected speed. Although not significant, the current study found that during stair ascending and descending, the obese group had shorter step length than the normal weight group, by 2.8% and 5.8% respectively. Since walking velocity was not controlled for, it was assumed that the velocity decreased with the step length proportionally.
Although not significant from the normal mass group, step width increased as step length decreased in the obese group. One potential cause of the larger step width could be the increase in the thigh diameter that prevents the obese group from placing their feet together. As the step width changes the obese group’s base of support changes. This is a requirement for many functional activities of daily life such as mobility and to avoid falling [10]. The gait pattern shows that obese adults tend to spend more time in the stance phase, which increases their stability [12]. Although not significant, the obese group tried to increase balance and stabilization by spending a longer time in the double stance position and thus less time in the swing phase.
The second hypothesis predicted that the obese group would have deviations from normal gait, seen with greater moments and forces than the normal mass group, which may contribute to injury of the of the lower extremity joints. Our hypothesis was partially supported. The obese group had a higher peak hip adduction moment during stair ascending than the normal mass group, by 0.34 Nm/kg. Strutzenberger et al., (2011) [17] documented that obese children had greater hip adduction and knee extension moments during stair ascending. This is similar to the increased hip adduction moment found during stair ascending in the current study. Strutzenberger et al., (2011) [17] found that children climbed the stairs with the same step width as normal mass children, which may be related to them not yet adapting their gait to maximize efficiency. The increased hip adduction moment that was found may have been caused by excess body mass in obese children. Although not significant, our study showed an increased step width in the obese group compared to normal mass group. The altered gait strategy with increased step width among the obese group may further explain why the hip adduction moments were significantly different between the two groups.
Excessive knee valgus from hip adduction increases the Q-angle because it displaces the patella medially relative to the tibial tubercle [3]. Similarly, this study reported that excessive hip internal rotation positions the patella more medially relative to the tibial tubercle. Based on this, it has been predicted that hip abductors and hip external rotator muscles weakness may cause excessive hip adduction and hip internal rotation, as seen in this study during stairs ascending.
In addition, significant differences were found between the obese and normal mass group in peak knee anterior shear forces during stairs ascending. The obese group had higher anterior shear force, by 0.67 N/kg. To the best of our knowledge, there is no previous research that has looked at the anterior shear force at the knee during stairs ascending, between obese and normal mass groups. These differences at the knee can be attributed to the location of the center of mass. It can be assumed that when ascending the stairs, the obese group may limit the use of the quadriceps and hamstring muscle groups to disperse the forces and as a result increase the shear force to control the forward movement.
In contrast to our hypothesis, peak hip adduction moment and peak knee abduction moment were higher at the normal mass group than the obese group during stairs descending, by 0.47 Nm/kg and 0.35 Nm/kg respectively. These findings may indicate that the obese group may be more restrict in their movements and range of motion while descending stairs than the normal mass group. It seems that the normal mass group has higher range of motion in the frontal plane than the obese group, trusting their muscle activation to support their body during the stairs descending.
Conclusion
Mobility is a critical component of everyday life. This study found a significant differences in the gait patterns between the normal massand obese groups. The findings from this study indicate that obese individuals adopt a different kinematic and kinetic gait strategy from initial contact to toe off. The strategy adopted by the obese group may be an attempt to better dissipate the larger ground reaction forces due to their increased mass. Future studies should be performed on a larger sample size to make definitive conclusions and analyze differences among the type of obese population.
References
- Anandacoomarasamy A, Fransen M, March L. Obesity and the musculoskeletal system. Current opinion in rheumatology. 2009 Jan 1;21(1):71-7.
- Andriacchi TP, Andersson GB, Fermier RW, Stern D, Galante JO. A study of lower-limb mechanics during stair-climbing. The Journal of bone and joint
surgery. 1980 Jul; 62(5):749-57.
- Bolgla LA, Malone TR, Umberger BR, Uhl TL. Hip strength and hip and knee kinematics during stair descent in females with and without patellofemoral pain syndrome. journal of orthopaedic & sports physical therapy. 2008 Jan; 38(1):12-8.
- Browning RC, Kram R. Effects of obesity on the biomechanics of walking at different speeds. Medicine & Science in Sports & Exercise. 2007 Sep 1; 39(9):1632-41.
- de Carvalho FR, Martins AT, Teixeira AM. Analyses of gait and jump tasks in female obese adolescents. Pediatric exercise science. 2012 Feb 1; 24(1):26-33.
- Costigan PA, Deluzio KJ, Wyss UP. Knee and hip kinetics during normal stair climbing. Gait & posture. 2002 Aug 1;16(1):31-7.
- de Souza SA, Faintuch J, Valezi AC, Sant'Anna AF, Gama-Rodrigues JJ, de Batista Fonseca IC, Souza RB, Senhorini RC. Gait cinematic analysis in morbidly obese patients. Obesity Surgery. 2005 Oct 1;15(9):1238-42.
- DeVita P, Hortobágyi T. Obesity is not associated with increased knee joint torque and power during level walking. Journal of biomechanics. 2003 Sep 1;36(9):1355-62.
- Felson DT. An update on the pathogenesis and epidemiology of osteoarthritis. Radiologic Clinics. 2004 Jan 1;42(1):1-9.
- Hills AP, Hennig EM, Byrne NM, Steele JR. The biomechanics of adiposity–structural and functional limitations of obesity and implications for movement. Obesity reviews. 2002 Feb;3(1):35-43.
- Kowalk D.L., Duncan J.A., Vaughan C.L. (1996) Abduction-adduction moments at the knee during stair ascent and descent. J Biomech. 1996 Mar;29(3):383-8. PubMed PMID: 8850644.
- Lai P.P., Leung A.K., Li A.N., Zhang M. Three-dimensional gait analysis of obese adults. Clin Biomech (Bristol, Avon). 2008;23 Suppl 1:S2-6. PubMed PMID: 18374462.
- McFayden, B.J., Winter, D.A. An integrated biomechanical analysis of normal stair ascent and descent. J Biomech. 1988;21(9):733-44. PubMed PMID: 3182877.
- Nadeau S, Gravel D, Hébert LJ, Arsenault AB, Lepage Y. Gait study of patients with patellofemoral pain syndrome. Gait & posture. 1997 Feb 1;5(1):21-7.
- Nantel, J., Brochu, M., Prince, F. Locomotor Strategies in Obese and Nonobese Children. Obesity (Silver Spring). 2006 Oct;14(10):1789-94. Pub- Med PMID: 17062809.
- Reid S.M., Lynn S.K., Musselman R.P., Costigan P.A. Knee biomechanics of alternate stair ambulation patterns. Med Sci Sports Exerc. 2007 Nov;39(11):2005-11. PubMed PMID: 17986909.
- Strutzenberger G., Richter A., Schneider M., Mündermann A., Schwameder H. Gait Posture. 2011 May;34(1):119-25. PubMed PMID: 21536442.
- Sturmer T, Gunther KP, Brenner H. Obesity, overweight and patterns of osteoarthritis: the Ulm Osteoarthritis Study. J Clin Epidemiol. 2000 Mar 1;53(3):307-13. PubMed PMID: 10760642.
- Wearing, S.C., Henning, E.M., Byrne, N.M., Steele, J.R., & Hills, A.P. Musculoskeletal disorders associated with obesity: a biomechanical perspective. Obes Rev. 2006 Aug;7(3):239-50. PubMed PMID: 16866972.
- Westlake CG, Milner CE, Zhang S, Fitzhugh EC. Do thigh circumference and mass changes alter knee biomechanics during walking? Gait Posture. 2013 Mar;37(3):359-62. PubMeb PMID: 22939753.





