Variations in Origin and Course of the Right and Left Coronary Arteries in Autopsied Hearts at the University Teaching Hospital, Lusaka, Zambia
Silitongo M1,2*, Zulu H1, Buumba PN1, Bowa K2, Erzingatsian K3, Kafumukache EB1
1 Department of Anatomy, School of Medicine, University of Zambia, Lusaka, Zambia.
2 Department of Basic Sciences, School of Medicine, Copperbelt University, Ndola, Zambia.
3 Departments of Surgery and Anatomy, School of Medicine, University of Zambia, Lusaka,Zambia.
*Corresponding Author
Moono Silitongo
School of medicine, Department of Anatomy,
University of Zambia, Lusaka, Zambia.
E-mail: moonosilitongo@gmail.com
Received: September 07, 2016; Accepted: October 18, 2016; Published: October 24, 2016
Citation: Silitongo M, Zulu H, Buumba PN, Bowa K, Erzingatsian K, et al., (2016) Variations in Origin and Course of the Right and Left Coronary Arteries in Autopsied Hearts at the University Teaching Hospital, Lusaka, Zambia. Int J Anat Appl Physiol. 2(6), 57-62. doi: dx.doi.org/10.19070/2572-7451-160009
Copyright: Silitongo M© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: Coronary arteries play an important role in perfusion of the heart tissues. Variations or anomalies in coronary arteries may be asymptomatic while some can be symptomatic and even cause sudden death. Knowledge of coronary artery variations is important in diagnosis and treatment of cardiovascular diseases.
Aim: To describe coronary artery anomalies and their incidence in autopsy cases.
Materials and Methods: We dissected and grossly examined a total of 127 human hearts during autopsy to describe coronary artery variations in origin and course.
Results and Conclusion: The incidence of coronary artery anomalies was found to be 4.72% (6/127; 1 female and 5 males). Among the coronary artery anomalies were: Absent left main coronary artery (LMCA) in 0.8% (1/127), origin of both the left and right coronary arteries from a common ostium located in the left aortic sinus in 0.8% (1/127), origin of both the left and right coronary arteries from a common trunk whose ostium was located in the right aortic sinus in 0.8% (1/127), origin of both the left and right coronary arteries from a common ostium located in the tubular part of the ascending aorta just above the right aortic sinus (RAS) in 0.8% (1/127), origin of the left coronary artery from a separate ostium in the RAS in 0.8% (1/127), origin of the right coronary artery from the sinutubular junction of the LAS in 0.8% (1/127) of the hearts.
Conclusion: The incidence of coronary artery anomalies in autopsied hearts was found to be 4.72%. Knowledge of the normal and variant anatomy of coronary arteries is indispensable and imperative both in diagnosis, treatment and implementation of interventional measures.
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Conclusion
7.Acknowledgements
8.References
KeyWords
Coronary Ostium; Aortic Sinus; Coronary Arteries; Coronary Artery Anomalies.
Introduction
Coronary artery anomalies are rare [1-3] though Anderson [4] in Grants Atlas of Anatomy states that the coronary circulation is extremely variable in detail. Coronary artery anomalies have a documented incidence range of between 0.26 % to 5.64 % in studies done using different methods in different countries [1,5-12]. Altin et al., [12] reported that the incidence of coronary artery anomalies (CAAs) varies from 0.2% to 8.4%. With the increase in the rate of cardiovascular diseases in developing countries [13] and Sub-Saharan Africa [14], knowledge of the normal and possible variations in the origin and course of the coronary arteries is indispensable and imperative in diagnosis, treatment and implementation of interventional measures [3, 15, 16]. Knowledge of the possible variations in the origin and course of the major coronary arteries can greatly enhance clinical outcomes [3]. Recognition and knowledge of coronary artery anomalies is important when performing angiographies and ensuring accurate angiographic interpretation [7, 16].
Materials and Methods
This study was done between September 2015 and February 2016 at the University Teaching Hospital (UTH), Lusaka, Zambia. A total of 127 human hearts (96 males and 31females, aged between 17 and 86 years) were dissected and grossly examined during autopsy offorensic cases i.e. road traffic accidents (RTA). The aim of this study was to investigate the incidence of anomalous origin and course of the coronary arteries in autopsy cases. Dissections were done by a Pathologist and two Anatomy postgraduate students. Photographs were taken after dissection using a digital camera Canon power shot SX400IS 16 mega pixels. Ethical clearance was granted by Excellence in Research Ethics and Science (ERES CONVERGE).
Results
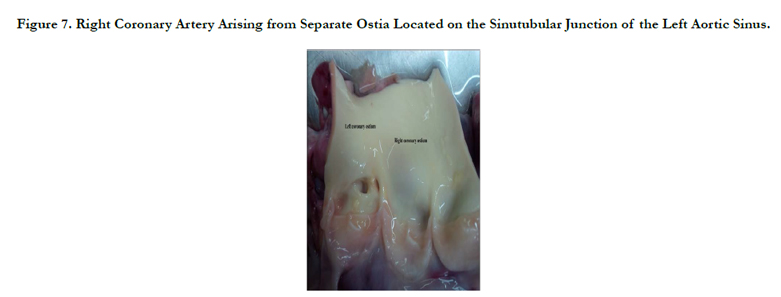
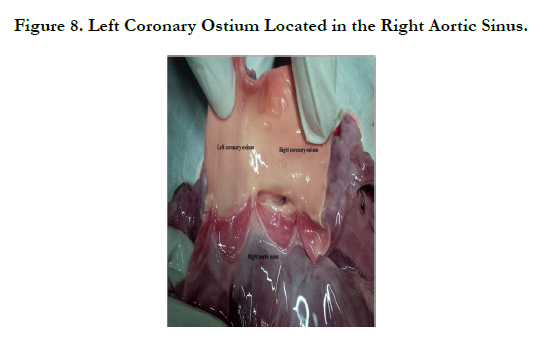
Coronary artery anomalies were found in 6 (1 female and 5 males) out of the 127 hearts dissected and examined during autopsy. Therefore the incidence of coronary artery anomalies was 4.72%. Coronary artery anomalies encountered in our study were: absent left main coronary artery (LMCA) in 0.8% (1/127), origin of both the left and right coronary arteries from a common trunk whose ostium was located in the right aortic sinus (Figures 1-3) in 0.8% (1/127), origin of both the left and right coronary arteries from a common ostium located in the tubular part of the ascending aorta just above the right aortic sinus (Figure 4) in 0.8% (1/127), origin of both the left and right coronary arteries from a common ostium located in the left aortic sinus (Figures 5, 6) in 0.8% (1/127), origin of the right coronary artery from the sinutubular junction of the left aortic sinus (Figure 7) in 0.8% (1/127), origin of the left coronary artery from a separate ostium in the right aortic sinus (Figure 8) in 0.8% (1/127) of the hearts.




Discussion
Congenital coronary artery anomalies of origin and course were found in 6 (4.72%) of the 127 hearts dissected during autopsy. In Texas in The United States of America, Angelini et al., [8] investigated 1950 angiograms from which they found the incidence of coronary artery anomalies at 5.6%. A study done in the United States of America at the University of Florida by Von Ziegler et al., [10] found the incidence of these coronary artery anomalies in 2.3% (17/748) consecutive symptomatic patients, who underwent cardiac 64-slice multi-detector-row computed tomography angiography (MDCTA). Kardos et al., [7] analysed angiographic data of 7,694 consecutive patients who underwent coronary arteriography at the Albert Szent-Gyorgyi Medical University, Szeged, Hungary, from 1984 to 1994 and found congenital coronary anomalies (CCA) in 103/7,694 patients (1.34% incidence). The incidences of coronary artery anomalies are summarised in Table 1. The variations in incidences of coronary artery anomalies have been attributed to ethnicity, racial differences [17] geographic region [3]. Abnormal arrangement of coronary arteries maybe associated with minor genetic changes in certain growth factors [3, 18]. Though the incidence of CAA from our study falls within the range of incidence of CAA, the percentage is higher and could be attributed to the smaller sample size we used when compared to the sample sizes of the other studies (Table 1).


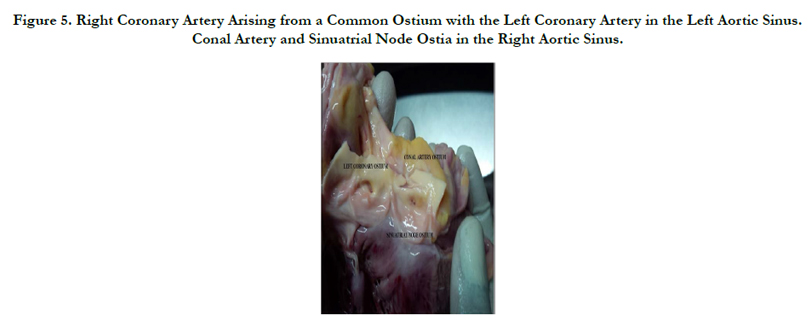
Among the CAA in our study was absence of left main coronary artery (LMCA) 1 (0.79%) of the hearts. In a study done by Ajayi et al., [19] in South Africa the LMCA was absent in 9.6% (39/407). Our observed percentage of this rare anomaly in our study falls within the 0.6-1.6% range stated by Papadopoulos et al., [20] in cases diagnosed by cardiac catheterisation in Greece. In Turkey, Altin et al., [12] found this anomaly in 0.9% (51/5548) patients who had undergone coronary angiography. Angelini et al., [8] found the incidence of absence of the left main trunk in 13/1950 (0.67%) angiograms. The right coronary artery arose from a common ostium with the left coronary artery in the left aortic sinus (Figure 5) in 1/127 (0.8%) hearts and on the sinutubular junction of the left aortic sinus (Figure 7) in 1/127 (0.8%) hearts. An exact percentage incidence (1.6%) of origin of right coronary artery from the left aortic sinus to what we found was reported by Jim et al., [21] among patients with first time cardiac catheterization. In other studies this CAA was found in: 0.026% (5/18950) by Alexander and Griffiths [1], 0.92% (18/1950) by Angelini et al., [8], 0.94% (7/748) by Von Ziegler et al., [10]. Matsumura et al., [22] also documented this anomaly after treating a patient who presented with sudden cardiac arrest associated with an anomalous right coronary artery originating from the left sinus of Valsalva. In Israel, Yuan et al., [23] diagnosed this coronary artery anomaly in a patient who presented with chest pain.
The left coronary artery arose from a separate ostium in the right aortic sinus (Figure 8) in 0.8% (1/127) hearts. In the study done by Angelini et al., [8] this anomaly was seen in 0.15% (3/1950) angiograms while Alexander and Griffiths [1] found this anomaly in 0.011% (2/18950) hearts in an autopsy based study. Anomalous origin of the coronary artery from the opposite aortic sinus with a course between the ascending aorta and the pulmonary artery can cause myocardial ischemia, syncope and sudden cardiac death in youngpeople especially during exercise. Other symptoms include dyspnoea, palpitations, angina pectoris and dizziness [24, 25]. Cheitlin et al., [26] suggested that the mechanism for sudden death in these cases is as a result of the acute leftward passage of the coronary artery along the aortic wall which causes the entrance into the left coronary system to be slit-like and that under circumstances of increased cardiac activity with increased expansion of the pulmonary artery and aorta with exercise, there is stretching of the left coronary artery and a flap-like closure of the orifice of the left coronary with sudden, fatal myocardial ischemia.
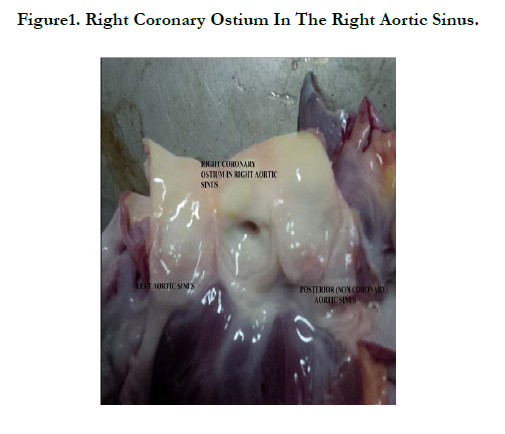
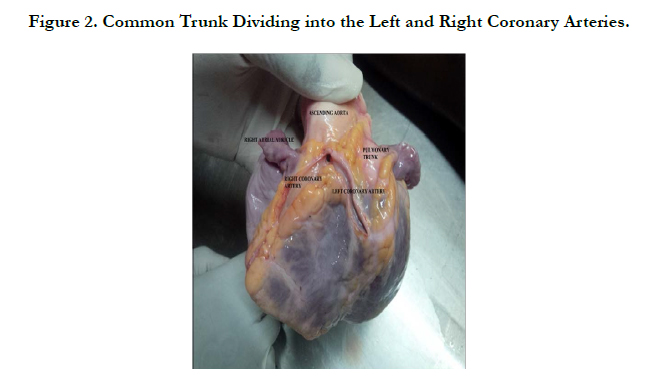
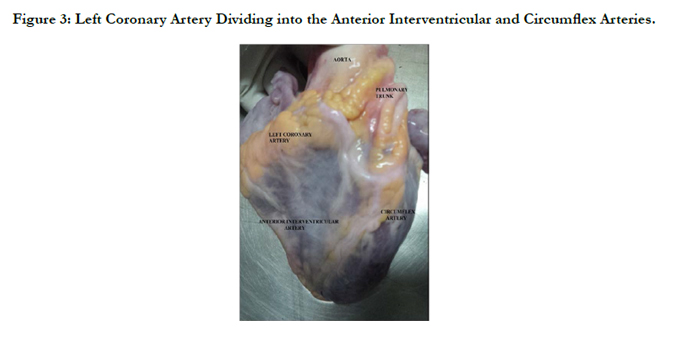
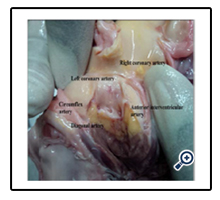
Single coronary artery (Figures 1 – 3) was seen in 0.8% (1/127) hearts. Angelini [25] described a similar case as single coronary ostium. The common trunk arose from the right aortic sinus (Figure 1), coursed anteriorly between the right auricle and the pulmonary trunk where it divided into the right and left coronary arteries (Figure 2). The left coronary artery coursed to the left off the common trunk between the ascending aorta and the pulmonary trunk and divided into the anterior interventricular and circumflex arteries (Figure 3). The right coronary artery coursed to the right off the common trunk anterior to the right auricle to the right cardiac border. According to Angelini et al.,[8] even though the common trunk arose from the right aortic sinus, it cannot be named as the right coronary artery but should be considered as a common mixed trunk from which arose both the right and left coronary arteries. Ogden and Goodyer [27] described single coronary artery as not the absence of a complete coronary artery, but rather the absence of a portion of one of the coronary arteries at the aortic root. Waller et al., [28] described single coronary artery as origin of the entire coronary circulation from a single aortic ostium as in our case. Angelini [25] described a similar case and named it as single coronary ostium since both coronary arteries are present. This CAA was also documented by Nerantzis and Koutsaftis [29]. Lipton et al., [30] described isolated single coronary artery as a rare anomaly occurring in approximately 0.024% of the population. Any congenital or acquired obstructive disease in the common trunk would deprive the heart muscle of nutrient rich blood since both coronary arteries arise from it and thus the heart muscle would become ischaemic without having any possible source of collateral circulation [8]
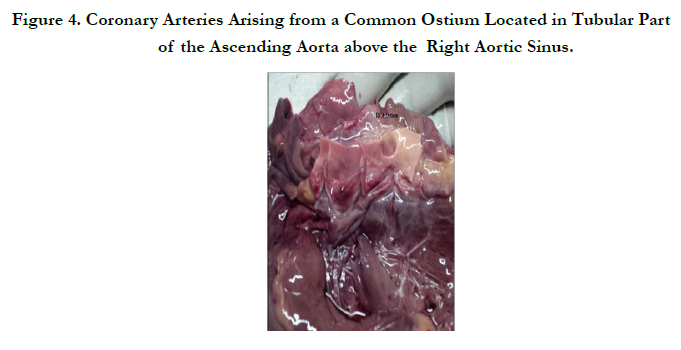
In 0.8% (1/127) hearts, both the right and left coronary arteries arose a common ostium located in the tubular part of the ascending aorta just above the right aortic sinus (Figure 4). Most studies published on this anomaly involve high origin (high take off) of only the right coronary artery. Piegger et al., [31] reported a case in which the right coronary artery arose from the ascending aorta 38mm above the supravalvular ridge. Nerantzis and Marianou [32], reported an anomaly in which in one heart both left and right coronary arteries arose from the left aortic wall 7 mm and 19 mm respectively above the sinutubular junction among 510 human hearts they examined. In our case the left coronary artery coursed high up in the cleft between the ascending aorta and the pulmonary trunk avoiding possible compression and similarly to their case the right coronary artery also avoided possible compression. The cardiac surgeon should be aware that high cannulation will be required to locate the right coronary artery to avoid accidentally cross-clamping or transecting the vessel during surgery where this anomaly may be encountered [32]. Singh [15] reported a case in which the right coronary artery arose from the anterior part of the ascending aorta 3 mm from its root. Lee et al., [33] also reported a case in which the right coronary artery arose from the ascending aorta above the left sinus of Valsalva and coursed between the aorta and pulmonary trunk. High take-off positions are without any haemodynamic significance, but they may lead to unexpected angiographic problems while localizing and engaging the orifices [34]. Knowledge of location of coronary ostium in aortic sinus is essential while manipulating a catheter in procedure of angiography, angioplasty and transcatheter aortic valve replacement procedures [17].
Conclusion
The incidence of coronary artery variations in origin and further proximal course was found to be 4.72%. Most variations seen were of origin though despite having anomalous origin, the coronary artery would still assume its normal course. Knowledge of the origin (location of coronary ostia), course and variations of the coronary arteries is important for radiologists performing angiographies for diagnostic purposes and also for cardiac surgeons implementing interventional and therapeutic measureswhen managing cardiovascular diseases. Attention to variations in the origin and course of the coronary arteries can greatly enhance clinical outcomes. This information may also be helpful when diagnosing and treating of cardiovascular diseases with the installation of computed tomography angiography equipment at the University Teaching Hospital, Lusaka, Zambia.
Acknowledgements
The authors would like to acknowledge the families who allowed us to use their deceased`sbodies in our research.
References
- Alexander RW, Griffith GC (1956) Anomalies of the Coronary Arteries and their Clinical Significance. Circulation. 14(5):800-805.
- Hauser M (2005) Congenital anomalies of the coronary arteries. Heart. 91(9):1240–1245.
- Loukas M, Groat C, Khangura R, Owens DG, Anderson RH (2009) The Normal and Abnormal Anatomy of the Coronary Arteries. Clin Anat. 22(1): 114–128.
- Anderson JE (1983) Grants Atlas of Anatomy. (8nd Edn), Lippincott Williams and Wilkins, New York.
- Yamanaka O, Hobbs RE (1990) Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 21(1): 28–40.
- Topaz O, DeMarchena EJ, Perin E, Sommer LS, Mallon SM, et al., (1992) Anomalous coronary arteries: Angiographic findings in 80 patients. Int J Cardiol. 34(2): 129 – 138.
- Kardos A, Babai L, Rudas L, Gaal T, Horvath T, et al., (1997) Epidemiology of Congenital Coronary Artery Anomalies: A Coronary Arteriography Study on a Central European Population. Cathet Cardiovasc Diagn. 42(3): 270–275.
- Angelini P, Villason S, ChanAV, Diez JD (1999) Normal and anomalous coronary arteries in humans. In: Angelini P, ed. Coronary Artery Anomalies: A Comprehensive Approach. Philadelphia: Lippincott Williams & Wilkins.27–150.
- Srinivasan K, Gaikwad A, Kannan B, RiteshK, Ushanandini K (2008) Congenital coronary artery anomalies: Diagnosis with 64 slice multidetector row computed tomography coronary angiography: A single-centre study. J Med Imaging Radiat Oncol. 52(2): 148–154.
- Von Ziegler F, Pilla M, McMullan L, Panse P, Leber AW, et al., (2009) Visualization of anomalous origin and course of coronary arteries in 748 consecutive Symptomatic patients by 64-slice computed tomography angiography. BMC Cardiovasc. Disorders. 9: 54.
- Graidis C, Dimitriadis D, Karasavvidis V, Karakostas G, Giannadaki M, et al., (2013) Prevalence and characteristics of coronary artery anomalies in 12401 adult patients: a coronary angiographic study from Northern Greece.
- Altin C, S Kanyilmaz S, Koc S, Gursoy YC, Bal U, et al., (2014) Coronary anatomy, anatomic variations and anomalies: a retrospective coronary angiography study. Singapore Med J. 56(6): 339-45.
- Okrainec K, Banerjee DK, Eisenberg MJ (2004) Coronary artery disease in the developing world. Am Heart J. 148(1): 7–15.
- Atadzhanov M, Mwaba M, Mukomena PN, Lakhi S, Mwaba P, et al., (2014) Frequency of APOE, MTHFR and ACE polymorphismsin the Zambian Population. BMC Res Notes. 7: 194.
- Singh R (2013) An Anomalous Configuration of Coronary Artery: A Cadaveric Study. Case Reports Cardiol. 2013: 397063.
- MamathaY, Sridhar C (2014) Anomalous Branching Pattern of Coronary Vessels. J Surg. 3:169-173.
- Kulkarni JP, Paranjpe V (2015) Topography, morphology and morphometry of coronary ostia - a cadaveric study. Eur J Anat. 19: 165-170.
- Walker W, Webb G (2001) Congenital coronary artery anomalies: The adult Perspective. Coron Artery Dis. 12(8): 599 – 604.
- Ajayi NO, Lazarus L, VankerEA, Satyapal KS (2014) Absent Left Main Coronary Artery with Variation in the Origin of its Branches in a South African Population. Anat Histol Embryol. 44(2): 81-85.
- Papadopoulos PD, Moyssakis I, Athanasiou A, Anagnostopoulou S, Benos I, et al., (2006) Right Coronary Ostium Agenesis with Absence of the Right Coronary Artery: A Rare Case of Non-ST Elevation Coronary Syndrome.Clin Anat. 19: 345–346.
- Jim MH, Siu CW, Ho HH, Miu R, Lam YM, et al, (2005) Anomalous origin of right coronary artery from the left coronary sinus: incidence, characteristics and a systematic approach for rapid diagnosis. J Interv Cardiol.18: 101-106.
- Matsumura K, Matsumoto H, Hata Y, Ueyama T, Kinoshita T, et al., (2016) Anomalous Right Coronary Artery Arising from the Left Sinusof Valsalva in a Young Athlete. Intern Med. 55(1): 55-58.
- Yuan SM, TagerS, Raanani E (2009) Anomalous Origin of the Right Coronary Artery from the Left Coronary Sinus. Chang Gung Med J. 32: 455- 458.
- Angelini P (2002) Coronary artery anomalies--current clinical issues: definitions, classification, incidence, clinical relevance, and treatment guidelines. Texas Heart Institute Journal 29(4) 271-278.
- Angelini P (2007) Coronary artery anomalies: an entity in search of an identity. Circulation. 115(10): 1296-1305.
- Cheitlin MD, De Castro CM, McAllister HA (1974) Sudden death as a complication of anomalous left coronary origin from the anterior sinus of Valsalva, a not-so-minor congenital anomaly. Circulation. 50(4): 780–787.
- Ogden JA, Goodyear AVN (1970) Patterns of distribution of the single coronary artery. Yale J Biol Med. 43(1): 11- 21.
- Waller BF, Orr CM, Slack JD, Pinkerton CA, TasselmJV, et al., (1992) Anatomy, Histology and Pathology of Coronary Arteries: A Review Relevant to New Interventional and Imaging Techniques-Part III. Clin Cardiol. 15: 607-615.
- Nerantzis CE, Koutsaftis PN (1998) Variant of the Left Coronary Artery with an Unusual Origin and Course: Anatomic and Postmortem Angiographic Findings. Clin Anat. 11(6): 367-371.
- Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L (1979) Isolated Single Coronary Artery: Diagnosis, Angiographic Classification, and Clinical Significance. Radiology. 130(1): 39-47.
- Piegger J, Kovacs P, Ambach E (2001) Extremely High Origin of the Right Coronary Artery from the Ascending Aorta. Clin Anat. 14(5): 369 –372.
- Nerantzis CE, Marianou SK (2000) Ectopic “High” Origin of Both Coronary Arteries From the Left Aortic Wall: Anatomic and Postmortem Angiographic Findings. Clin Anat.13(5): 204–206.
- Lee J, Kim D, Byun S, Choi W, Lee C, et al., (2009) A Case of Acute Myocardial Infarction with the Anomalous Origin of the Right Coronary Artery from the Ascending Aorta above the Left Sinus of Valsalva and Left Coronary Artery from the Posterior Sinus of Valsalva. Yonsei Med J. 50(1): 164 – 168.
- Zeina AR, Blinder J, Sharif D, Rosenschein U (2009) Congenital coronary artery anomalies in adults: non-invasive assessment with multidetector CT. Br J Radiol. 82(975): 254–261.





