Histomorphological Spectra of Gallbladder Specimens after Cholecystectomy in Benign Disease
Gaharwar A1, Mishra SR1*, Kumar V2
1 Department of Anatomy, Ganesh Shankar Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India.
2 Department of Anatomy, Rural Institute of Medical Science and Research, Saifai, Uttar Pradesh, India.
*Corresponding Author
Suniti R Mishra
Professor, Department of Anatomy, G.S.V.M. Medical College,
Kanpur, Uttar Pradesh, India.
Tel: 09959994994
E-mail: dr.sunti@yahoo.co.in
Received: July 05, 2016; Accepted: August 24, 2016; Published: August 31, 2016
Citation: Gaharwar A, Mishra SR, Kumar V (2016) Histomorphological Spectra of Gallbladder Specimens after Cholecystectomy in Benign Disease. Int J Anat Appl Physiol. 2(5), 49-56. doi: dx.doi.org/10.19070/2572-7451-160008
Copyright: Mishra SR© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Background: The gallbladder is a surgically important organ, most often subjected to cholecystectomy for treating cholelithiasis. The presence of gallstones may precipitate the development of cholecystitis which may even lead to gallbladder malignancy, if not treated in time.
Aim: The aims were to study the diverse morphological, histopathological and histochemical features of gallbladder specimens
obtained at cholecystectomy done for various benign diseases of the GB.
Material and methods: Included are 132 specimens of the gallbladder obtained at cholecystectomy done for benign diseases at Ganesh Shankar Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India. The specimens thus obtained were studied for the morphological and histopathological changes. Each specimen was subjected to Sudan Black B, Methyl Green-Pyronin Y and Periodic acid-Schiff staining to confirm presence of lipid, plasma cells and glycogen, respectively in GB tissue samples.
Results and Conclusion: Cholelithiasis was predominantly a female disease. The size of the GB varied from < 7 cm (shrunken) to > 10 cm (distended). Cholelithiasis was present in 97.73% of the cases studied. Of these, 89.14 % had mixed stones and 10.85%, cholesterol stones. Of the cases studied, 8.33% had acute cholecystitis alone. It was associated with mucocoele or empyema of the GB in 3.79% and 5.30% cases, respectively. Histopathological changes consistent with chronic cholecystitis and cholesterolosis, respectively were seen in 76.52% and 6.06% cases. In the former patients, the presence of theplasma cells in the GB tissues was confirmed using MGPY staining. The presence of lipids in the GB tissue samples of the latter was confirmed using Sudan Black B staining. Cases of chronic cholecystitis with ectopic pancreatic tissue, colonic metaplasia and xanthogranuloma were also seen. Mixed atrophic-hyperplastic mucosa, being the commonest mucosal change was seen in 63.64% cases.Other mucosal changes included atrophic mucosa (in 21.21 % cases) and hyperplasia (in 15.15% cases).The GB tissue samples in 7.5% cases showed PAS-positive mucinous metaplasia.
The tissue samples obtained at cholecystectomy performed for various benign gallbladder diseases showed varieties of histomorphological changes, including metaplasia and precursor changes suggesting the high risk for gallbladder malignancy. This underscores the need for routine histopathological examination of appropriate tissue samples of the gallbladder obtained at cholecystectomy.
2.Introduction
3.Materials and Methods
4.Results
5.Discussion
6.Conclusion
7.References
KeyWords
Cholecystitis; Cholelithiasis; Empyema; Gallstone; Mucosa; Mucocoele.
Introduction
Disorders of the gallbladder are a common surgical condition throughout the world. Cholecystectomy is the mainstay of treatment for cholelithiasis and the laparoscopic cholecystectomy is the gold standard management of symptomatic cholelithiasis [1, 2]. Chronic cholecystitis is associated with cholelithiasis in > 90% of cases [3]. Although symptomatic cholelithiasis per se is a benign condition, gallstones are a known risk factor for gallbladder malignancy (GBM) which has a very poor prognosis [2-4]. Cholelithiasis produces diverse histopathological changes in the gallbladder. These include acute or chronic inflammation, xanthogranulomatous cholecystitis, glandular hyperplasia, cholesterosis, and metaplasia (gastric or intestinal), dysplasia and carcinoma [3]. The incidence of the gallbladder cancer varies in different races and geographic regions [3, 5]. The incidence is relatively high in North India, Pakistan, East Asia, Eastern Europe, and South America [6, 7]. In India, there is a distinct female (2.3 versus 1.01) dominance in the incidence (per 100,000 population) of GBM [8, 9].
Untreated cholelithiasis is a potentially serious condition as it may lead to life-threatening complications. The study presented herein aimed at identifying various morphological, histopathological and histochemical changes as might be found in tissue samples obtained at cholecystectomy done for various benign diseases of the GB.
Materials and Methods
The study was the product of a collaborative work involving the Department of Anatomy, the Department of General Surgery and the Department of Pathology, Ganesh Shankar Vidyarthi Memorial Medical College, Kanpur, Uttar Pradesh, India. It was a retrospective, observational study examining 132 tissue samples of the GB obtained at cholecystectomy performed at the Department of Surgery. Included were the tissue samples of the GB obtained from only those patients (121 females and 11 males) diagnosed having benign GB disease. Not included were the tissue samples of the GB obtained from those having GB malignancy.
The tissue samples of the GB were fixed in 10 per cent formalin. Prior to this, the gross appearance of the GB, presence or absence of any calculus and the color of any calculus, if present was noted. Then specimens were sectioned serially at the fundus, body and neck. Routine processing of tissues sections and staining with haematoxylin and eosin were done and examined. The histopathological examination of mucosa of the GB was done with special care. Special staining with Sudan Black B, Methyl- Green Pyronin Y stain and Periodic acid - Schiff (PAS) stain was also done in all cases for the demonstration of lipids, plasma cells and glycogen, respectively.
Results
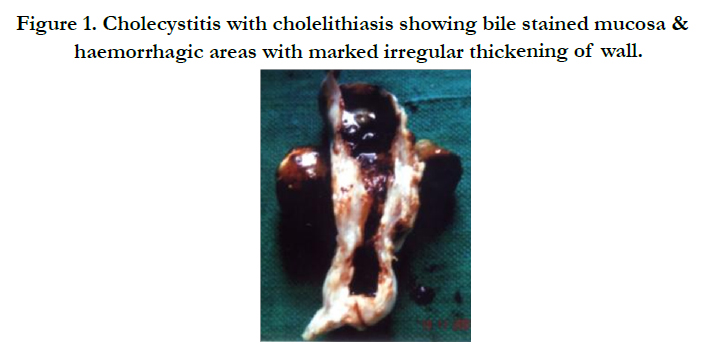
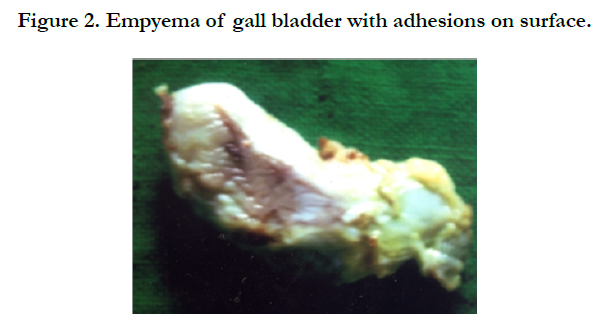
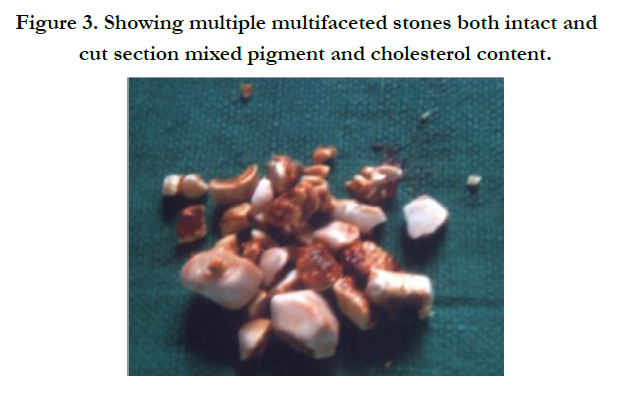
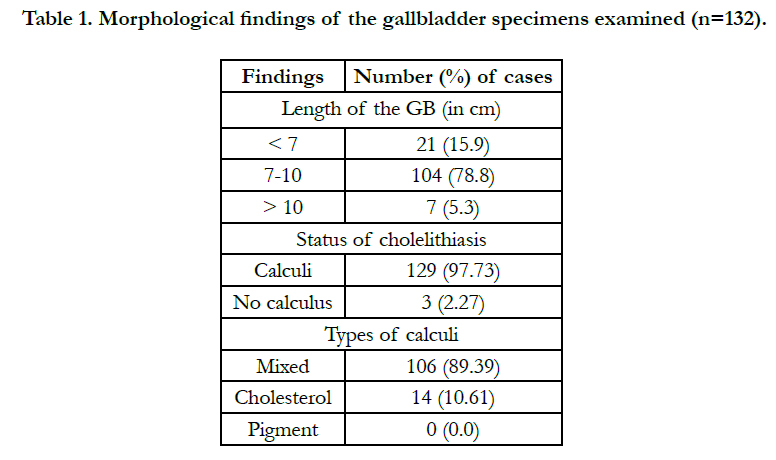
Of the total 132 patients underwent cholecystectomy, 121 were females and 11,males. Hundred and four (78.8%) GBs were 7-10 cm, 21 (15.9%), < 7cm and 7 (5.3%), > 10 cm in size. Calculi were found in 129 of 132 (97.73%) of GBs removed (Figure 1). Concomitant mucocele and empyema of the GB, respectively was found in 5 and 7 cases (Figure 2). No stone was found in 3(2.27%) cases. This subset included two males and one female. Mixed stones and cholesterol type stones (Figure 3) were present in 106 (89.14%) and 14 (10.85%) specimens, respectively. Pigment
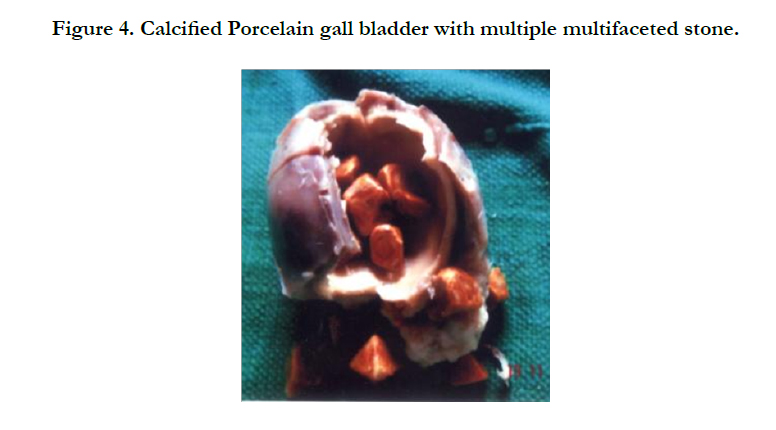
stones were not seen in any specimen (Table 1). Porcelain GB with the calcified wall was found in 1 case (Figure 4).



Histopathological features of chronic cholecystitis (Figure 5) with or without associated cholesterolosis were seen in 101(76.52%) and 8 (6.06%) specimens, respectively. Acute cholecystitis alone was found in 11 (8.33%) cases (Table 2). Five (3.79%) cases of acute cholecystitis had associated mucocele of the GB. Seven (5.30%) had associated empyema of the GB.
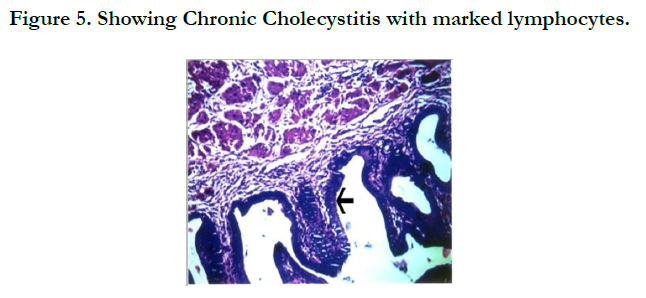
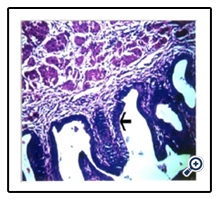
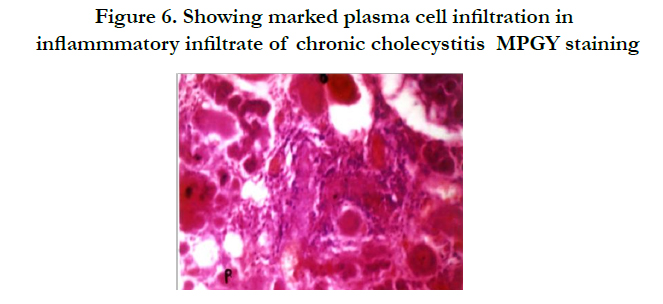
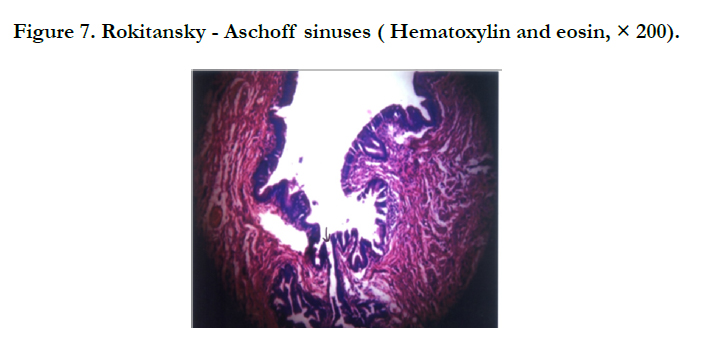
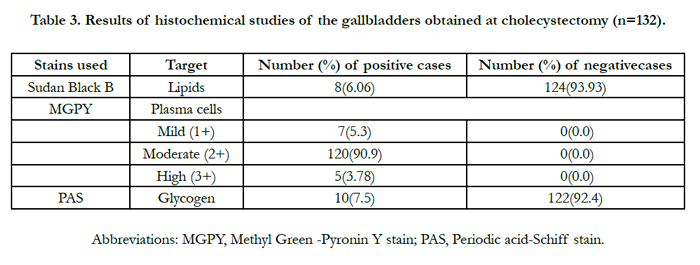
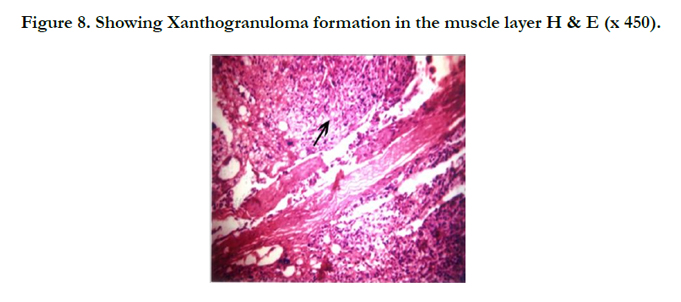
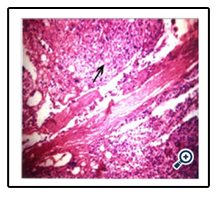
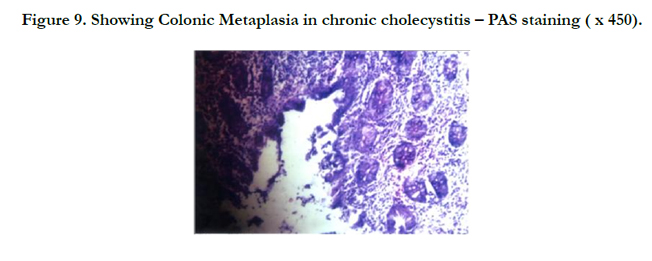
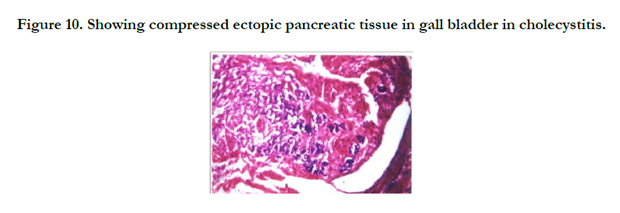
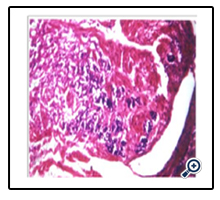
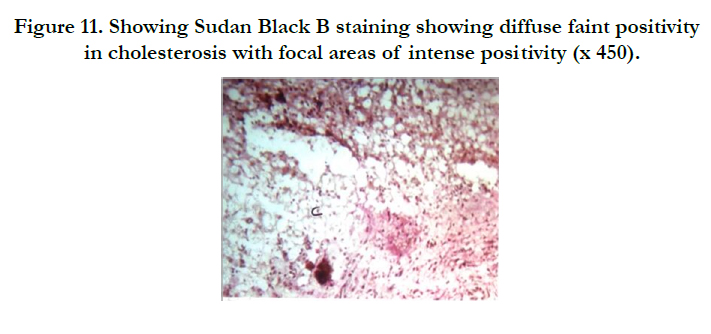
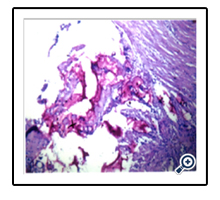
When present, the chronic inflammatory infiltrate was characterized by the presence of scattered lymphocytes, plasma cells and macrophages. The marked plasma cell infiltration in the inflammatory infiltrates of chronic cholecystitis was confirmed using MGPY staining (Figure 6), which showed (Table 3) high (in 5 cases), moderate (in 120 cases) , and mild (in 7 cases) degree of positivity for plasma cell infiltration. Sub-epithelial and sub-serosal fibrosis and Rokitansky-Aschoff sinuses were also prominent (Figure 7). A case of xanthogranulomatous cholecystitis was seen in which abundant lipid-laden macrophages and exuberant tissue fibrosis were present (Figure 8). Colonic metaplasia was seen with PAS staining (Figure 9). A rare case of compressed ectopic pancreatic tissue with chronic cholecystitis was also seen in the study (Figure 10).The histochemical confirmation of cholesterolosis (Table 3, Figure 11) was based on the presence ofsub-mucosal deposition of lipids and cholesterol (Sudan Black B staining).
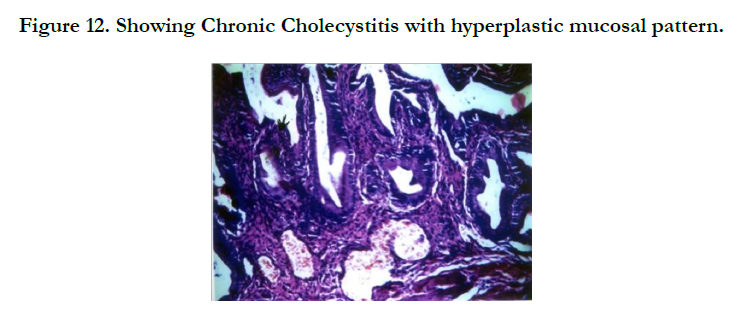
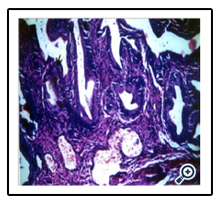
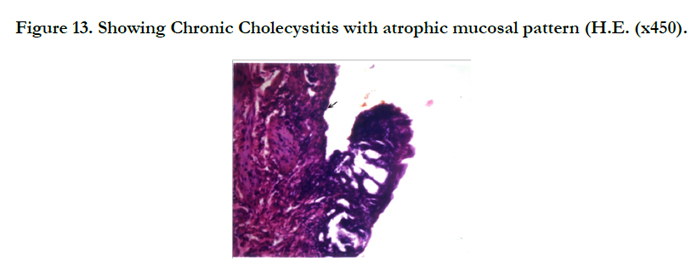
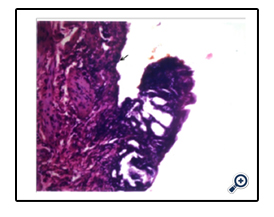
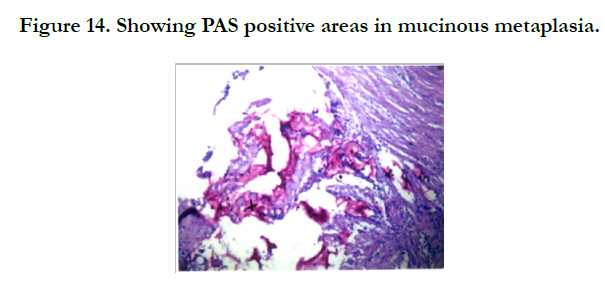
Hyperplastic GB mucosa was found in 20 (15.15%), atrophic mucosa, in 28 (12.21%) cases and mixed atrophic- hyperplastic mucosa, in 84 (63.64%) cases (Table 2, Figures 12, 13). Mucinous metaplasia (PAS-positive) was found in 10 (7.5%) cases; PAS staining was negative in 122 (92.4%) cases (Table 3, Figure 14). Histological features consistent with malignancy were uniformly absent in all specimens examined.
Discussion
Cholelithiasis (gallstone disease) is the most common surgical condition affecting the billary tract [10]. In the present study, females outnumbered males by a ratio of 11 to 1, a pattern similar to what has been noted by others [3]. This may not be surprising, considering the lithogenic effects of female sex hormones and the presence of estrogen and progesterone receptors inthe GB [9-11].
The GB was found fully relaxed and distended (measuring > 10 cm in length) in 7 (5.3%) cases. It was normal measuring 7- 10 cm in length [12-15] and shrunken measuring less than 7 cm in length in 104(78.8%) and 21 (15.9%) cases, respectively. Thus the functional status of the GB showed a varying range.
Mixed stones and cholesterol type stones were present in 106 (89.14%) and 14 (10.85%) specimens, respectively. Pigment stone was not found in any case. Our findings support those of others [11, 16]. Considering the cases in aggregates, stones were found in the GB in 129 of the 132 (97.7%) specimens examined (Figures 1-2). Associated mucocoele and empyema of the GB was found in 5 (3.79%) and 7 (5.33%) cases, respectively (Figure 3). Only 3(2.27%) specimens, taken from two males and one female patient, had no stone. We have found a rare case of porcelain GB with the dystrophic calcification of the GB wall.Of note, many consider [17] procelain GB a pre-malignant state. The diversities of the gross appearance of the GB found in the current study bear resemblance to the patterns reported by others [17-19]. In those reports, 49.7% of the GB specimens obtained at cholecystectomy were < 7 cm, 36.46%, 7-10 cm and 9.89%, > 10 cm in length.
We found histologically-proven acute cholecystitis in 18 (13.63%) cases; 5 cases (3.79%) had acute cholecystitis associated with mucocele of the GB. In total, 101 (76.52%) specimens showed histological features of chronic cholecystitis (Figure 5); chronic cholecystitis associated with cholesterolosis was found in 8 (6.06%) specimens. In one study [18], the majority (75%) of the postcholecystectomy GBs examined showed histological evidence of chronic cholecystitis. Relatively fewer cases [18] showed features of empyema (1.04%) and cholesterolosis (12.25%) of the GB.
Acute cholecystitis is a rare variant of cholecystitis and is characterized histologically by the presence of edema, hyperemia, extravasations of red blood cells and prominent fibroblastic proliferation. The process may be initiated by chemical irritations or bacteria-induced inflammation [20] probably triggered by the obstruction in the neck of the GB or the cystic duct by stones or edema of the surrounding tissues [2].
Mucocele of the GB has an incidence of 3 per cent [21]. In this study [21], 5(3.79%) cases of mucocele of the GB presented with features clinically simulating those of acute cholecystitis. All had an over-distended GB (>10 cm) filled by mucous. Histologic features were remarkable for flattened mucosa of the GB lined by low columnar or cuboidal cells, numerous RASs and inflammatory infiltrates.
In the current study, empyema of the GB was seen in 7(5.33%) cases (Figure 3). The key pathogenic factor is the unresolved cholecystitis induced by gallstones coupled with the bacterial contamination of the bile [22]. The other key factor is the bacterial contamination of the mucous accumulated in the GB [21]. The most frequently isolated bacteria species in such settings include Escherichia coli, Klebsiella pneumoniae, Streptococcus faecalis and anaerobe (e.g., Bacteroides and Clostridia species). The resulting suppurative inflammation packs the GB with purulent debris. The incidence of the surgically-proven (i.e., detected at chloecystyectomy) empyema of the GB varies widely from 2.4 to 11% [23, 24]. Empyema of gall bladder is often difficult to distinguish from uncomplicated acute cholecystitis [25].
Repeated bouts of mild to severe acute cholecystitis may result in chronic cholecystitis. In nine out ten cases, it is associated with cholelithiasis [26]. In the current study, none of the GB tissue samples examined showed any microscopic feature that could be considered normal. In one series [27], histologically normal GBs were found in less than one per cent of cases, when cholecystectomy was done for cholelithiasis. These data suggest that as claimed before, cholelithiasis was the commonest indication for cholecystectomy [11] (Figure 1). In one study, histologic evidence of chronic cholecystitis was found in more than half (50.8%) of the cholecystectomy specimens examined [28]. In another study [18], microscopic features of chronic cholecystitis were found in 64.8% of the GBs examined.
A distinctive feature of the GB is the presence of RASs, deep out-pouchings of mucosa which may extend through muscular layer [29]. The number of RASs is closely related to the degree of inflammation of the GB [27] as in chronic cholecystitis (Figure 5). Included in our series is a rare case of xanthogranulomatous cholecystitis in which gall bladder was shrunken, nodular and chronically inflamed with foci of necrosis and haemorrhages. The condition arises due to the rupture of RASs. This is a benign condition, though may be confused macroscopically with GBM because it infiltrates surrounding structures like the liver, the small and large intestine and the omentum [19, 30].
Cholesterolosis of the GB is the deposition of lipids and cholesterol esters in sub-epithelial cells, which project into lumen as polyps [26]. It affects mostly multiparous females [31]. In the current study, cholesterolosis was seen in 8 (6.06%) cases. All were females. Others found cholesterolosis in 2.7-12.3% of the GBs removed for benign diseases affecting the organ [18, 27].
The lumen of the GB is lined by columnar epithelium with microvilli [32]. Chronic irritations of the GB mucosa due to stones may lead to atypical cellular changesand hyperplasia, which may eventually progress to metaplasia and carcinoma-in-situ [33]. In the current study, the mucosal changes seen in the GB include mucosal hyperplasia in 20 (15.15%), mucosal atrophy in 28 (21.21%) and mixed atrophic variety in 84(63.3%) cases. Others found mucosal hyperplasia in as much as 25.3 % of the GBs examined [18]. One study reported epithelial hyperplasia having been found in 69% and antral metaplasia, in 16.5% of cases [30].
In the current study, mucinous metaplasia (i.e., PAS-positive colonic metaplasia with intra-cytoplasmic mucin) which many regard suggestive of borderline malignancy of the GB was in seen in 10 (7.5%) cases. We, as well as others [35], have found that ectopic pancreatic tissues in the GB associated with chronic cholecystitis due to cholelithiasisis a rare occurrence. Metaplasia of the GB mucosa induced by chronic cholecystitis is a pre-malignant condition. Although lacking confirmation, the pathogenesis of the mucosal dysplasia of the GB seen in chronic inflammation may involve loss of the heterozygosity of p53 gene and excessive expression of the gene [35].
Conclusion
Within the constraints of small sample size, we conclude that cholelithiasis was the commonest underlying reason for cholecystectomy in majority of cases of benign diseases of the gallbladder. The morphological appearance of the gallbladder varied from a shrunken, normal or distended organ with focal haemorrhages, sometimes filled with mucus or pus. The histopathological changes were equally diverse, showing features of acute and chronic cholecystitis, cholesterolosis, xanthogranuloma, dystrophic calcification, hyperplasia and metaplasia. Irrespective of the gross appearance and seemingly benign nature of the disease affecting the organ, every gallbladder removed by cholecystectomy should be subjected to
histopathological examinations.
References
- Jayasundara JASB, de Silva WMM (2013) Histological assessment of cholecystectomy specimens performed for symptomatic cholelithiasis: routine or selective Annals R Coll Surg Engl. 95 (5): 317-322. doi: 10.1308/0035884 13X13629960046471.
- Elwood DR (2008) Cholecystitis Surg Clin North Am. 88(6): 1241-1252. doi: 10.1016/j.suc.2008.07.008.
- Kafle SU, Sinha AK, Pandey SR (2013) Histomorphology spectrum of gall bladder pathology in cholecystectomy specimens with clinical diagnosis of chronic cholecystitis. J Nepal Med Assoc;52(192):600- 607.
- Sanders G, Kingsnorth AN (2007) Gallstones BMJ ; 335(7614):295-299.
- Symmers W. St. C Liver, biliary tract and exocrine pancreas; Vol eleven 3rd edition: 1984 chapter 9. 357-382.
- Royal College of Pathologists (2005) Histopathology and Cytopathology of limited or No clinical Value. 2nd edn. London: RCP file:///C:/Users/scidoc-001/Downloads/Histopathology_and_cytopathology_of_limited_or_no.pdf
- Russel RCG, Williams NSBlustrade GJK (2000)-Stones, Short practice of surgery, 23 edition Arnold Publisher. 1973-74.
- Behari A, Kapoor VK (2010) Does gallbladder cancer divide india ? Indian J Gastroenterol 29(1): 3-7. doi: 10.1007/s12664-010-0008-1.
- Singh G, Mathur Sk, Parmar P et al., (2016) Premalignant epithelial lesion of gall bladder: a histopathological study. Int J health Sci and Res 6(4):141-145.
- Shielasherlok (1997) Diseases of liver and Bilary system 10 edition. Wiley- Blackwell,USA.
- Zuhair R, Hani AB, Saleh M, Ansari AL (2011) Prevelance and Morphology and chemical composition of Gall stones The Iraqi Post graduate medical Journal vol. 10 No.1.
- Chari RS, Shah SA. (2008) Sabiston Textbook of Surgery, in Biliary system. 18th ed. secX , ch 54 WB Saunders St. Louis. 54. 1474-14.
- McGregor AL, Decker GAG, Plessis DJ Du (1986) Lee Mc Gregor's synopsis of surgical anatomy in the Liver and The Biliary System. 12th edn. KM Verghese and company, Bombay 78-103: 7.
- Moore KL and Dalley AF (2006) Clinically Oriented Anatomy in Abdomen. 5th edn, Lippincott Williams & Wilkins, Philadelphia, 302, 8.
- Vakili K, Pomfret EA (2008) Biliary anatomy and embryology. Surgical Clin of North America, 88(6); 1159-1174, doi: 10.1016/j.suc.2008.07.001.
- Alwan MH (1984) Incidence of cholelithiasis in Kuwait: A review of 894 cases Arab J. Med. 3: 17-20.
- Kalita D, Pant L, Singh S, Jain G, Kudesia M, Gupta K, Kaur C (2013) Impact of routine histopathological examination of gall bladder specimens on early detection of malignancy - a study of 4,115 cholecystectomy specimens, Asian Pac J Cancer Prev14 (5): 3315-8.
- Kaur A, Dubey VK, Mehta KS (2012) Gall Bladder mucosal changes associated with chronic cholelithiasis, Department of Pathology and Surgery ASCOM Sidhra, Jammu (J&K) India www.JK science vol 14 no. 2 April-June.
- Alumuslamani AJ, ALsoude M, Alomari M, Mnazel T, Khaswana G (2011) Histopathological examination on suspicious gall bladder specimens at Royal medical services hospital RMJ 36(2): 93-96.
- Kumar V, Abbas AK, Nelson F, Robbins and Cotron Pathologic basis of disease 7 edition, ELSEVIER SAUNDERS
- Rosai J (2004)Rosai and Ackerman's Surgical Pathology. 9th ed. New York, NY: Mosby;. vol 1: 1039. Published by Elsevier Mosby, St. Louis, MO, USA,2004.
- Wang CH, Chou HC, Liu KL, Lien WC, Wang HP, Wu YM (2013) Long- Term Outcome of Patients with Acute Cholecystitis Receiving Antibiotic Treatment: A Retrospective Cohort Study. World J Surg. 38(2): 347-54. doi:10.1007/s00268-013-2311-3.
- Thornton JR, Heaton KW, Espiner HJ, Espiner HJ, Eltringhan WK (1983) Empyema of the gall bladder - reappraisal of a neglected disease. Gut. 24 (12): 1183-1185.
- Horton R, Henry R (1984) Empyema of the gallbladder - a forgotten disease. Lancet. 17:1(8377):606.
- Taylor HW, Huang JK (2008) Routine pathological examination of gall bladder is a futile exercise. Br J Surg. 1998. 85(2): 208.
- Jacyna MR (1990) Interaction between Gall mucosa and bile; Relevance of Gall stone formation: GUT; 31: 568 –570.
- Tyagi SP, Tyagi N, Maheshwari v, Ashraj S M Sahoo P (1992) Morphological changes in diseased Gall Bladder a study of 415 cholecystectomy specimens in Aligarh. J Indian medical association 90(7): 178-81.
- Memon W, Khanzada TW, Samad A, Kumar B (2011) Histopathology spectrum of gall bladder specimen after cholecystectomy. Pak Journal Med. Sc.27(3): 533-536.
- Ross M, Pawlina W (2011) Histology: A Text and Atlas (6th ed.). Lippincott Williams & Wilkins. p. 646.
- Terada T (2013) Histological features and frequency of gall bladder lesions in consecutive 540 cholecystetomies, Int J Clin Exp Pathol. 6(1): 91-96.
- Junai R(1981) Surgical pathology Ackerman vol. 2 pg 1881, 7 edition.
- Young, Barbara, et al. (2006) Wheater's functional histology: a text and colour atlas (5th ed.). [Edinburgh]: Churchill Livingstone/Elsevier. p. 298
- Duarte I, Llanos O, Domke H, Harz C, Valdivieso V (1973) Metaplasia and precursor lesions of gall bladder carcinoma. Frequency,distribution and probability of detection in routine histologic samples. Cancer. 72 (6): 1878-1884.
- Elhence P, Bansal R, Agrawal N (2012) Heterotopic pancreas in gall bladder associated with chronic cholecystolithiasis Int J Appl Basic Med Res. 2(2): 142–143.
- Tazuma S, Kajiyama G (2001) Carcinogenesis of malignant lesion of the gall bladder. Lagenbeck’s, Arch Surg. 386 (3): 224-229.





