Towards A Successful Peritoneal Dialysis Program
Karkar A
Kanoo Kidney Centre, Dammam Medical Complex, Dammam, Saudi Arabia.
*Corresponding Author
Dr. Ayman Karkar, PhD, FRCP, FASN,
Department of Nephrology, Kanoo Kidney Centre, Dammam 31463, PO Box 11825, Kingdom of Saudi Arabia.
E-mail: aymankarkar@yahoo.com
Tel : 00966 13 891 2710
Fax : 00966 13 891 2610
Received: September 14, 2016; Published: September 20, 2016
Citation: Karkar A (2016) Towards A Successful Peritoneal Dialysis Program. Int J Chronic Dis Ther. 2(1e), 1-4. doi: dx.doi.org/10.19070/2572-7613-160005e
Copyright: Karkar A© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Keywords: Automated Peritoneal Dialysis; Hemodialysis; Renal Replacement Therapy; Chronic Kidney Disease; Education and Training.
Peritoneal dialysis (PD), hemodialysis (HD) and kidney transplantation constitute an integral renal replacement therapy program [1], where end-stage renal disease (ESRD) patients can be shifted to one or more of these treatment modalities according to their assessment and prescription and/or when one of these modalities fails to satisfy its needs [2]. PD has been well established as a first choice renal replacement therapy (RRT) modality with higher survival rate, especially in the first few years of treating ESRD patients [3]. PD, and in particular when there are no contraindications, can be an excellent initial choice and first treatment option (Table 1).
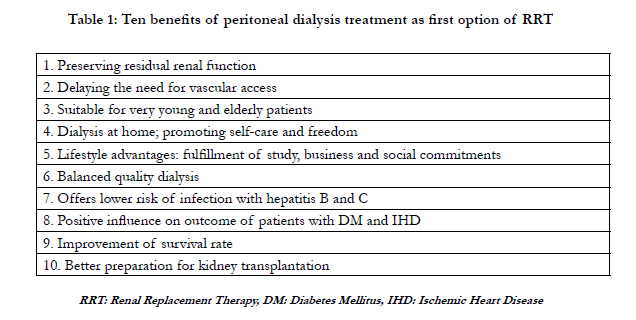

Table 1: Ten benefits of peritoneal dialysis treatment as first option of RRT
Multiple studies have shown that when compared to HD, PD is associated with equivalent or better survival especially among non-diabetic and younger diabetic patients, where PD has an equal or lower mortality rate during the first 1-2 years of therapy [3-6]. More recent studies have shown that PD and in center HD provide similar short and long term survival [7]. PD has the benefits of preserving residual renal function [8], delaying the need for vascular access and helping patients with multiple vascular access failure, and constitutes a better option for older age groups especially those with cardiovascular disease [8, 10]. PD has been associated with lower risk of infection with hepatitis B and C [11, 12], better outcome after transplantation with lower incidence of acute kidney injury and delayed graft function, lower costs than HD, and in promoting self-care and helping patients who are in need of more freedom [reviewed in 1]. In fact, PD has become an attractive modality of renal replacement therapy following the recent availability of new PD solutions such as icodextrin and amino-acid-based [13, 14] and biocompatible PD fluids [15]. The better understanding of the molecular mechanisms involved in solute and water transport across the peritoneum, the advances in PD technology, and in particular catheter placement [16], better connecting systems with significant reduction in peritonitis rate, and the improved technology of new generation of automated compact easy to use cyclers with many advantages (table 2) have enhanced PD utilization [7]. Studies from the United Kingdom [17] and studies from Netherlands, Belgium and New Haven study [18-20] have documented that if patients are given informed choice of dialysis treatment, 40-60% will choose PD modality. In addition, when comparing patient satisfaction with modality of HD versus PD as in CHOICE study, patients on PD therapy were more satisfied [21]. Furthermore, patients on PD modality from New Haven study were not only more satisfied with their care, but they also felt with less significant impact of PD on their lives [22].
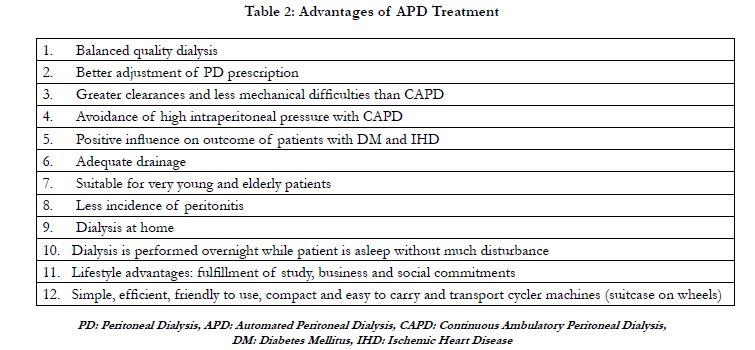
Table 2: Advantages of APD Treatment
The use of cyclers in North America has increased from 10% in 1990 to 54% in 2000 [23] and in Australia increased from 4% in 1995 to 42% in 2004 [24]. Furthermore, APD has grown steadily in different parts of the world and, for example, it accounts for 35% of the PD patients in Mexico [25]. Globally, it has been estimated that approximately one-third of PD patients are being maintained on APD treatment [26]. In contrast with continuous ambulatory peritoneal dialysis (CAPD), the efficacy of APD, especially in high and high-average peritoneal transport membranes [27], its higher [25] or similar [24, 28] patient and technique survival rates[2], reduced peritonitis rates [2, 25, 29, 30], similar extracellular fluid volume and blood pressure control and sodium removal [31] or enhanced ultrafiltration [32], avoidance of high intraperitoneal pressure and decreased mechanical complications [33], home therapy and improved quality of life with more freedom for patients to fulfill their employment and lifestyle [34], all of which enhanced the popularity of APD modality [35]. These advantages have been shown in HD patients transferred to APD [2], and confirmed even for anuric patients as demonstrated in the European Automated Peritoneal Dialysis Outcome (EAPOS) Study [36].
However, despite these multiple benefits and advantages there hasn’t been much progress [37] but rather a decline in PD utilization in several countries. The penetration rate of PD worldwide is about 11% [35, 38]. PD modality has been declining in most developed countries[39, 40] but increasing in developing countries[35, 41]. In United States, the use of PD has increased appreciably in recent years (7.4% of patients with a known dialysis modality). This change is associated with the new bundled payment system, with its clear incentives for peritoneal dialysis [42]. Likewise, allowing reimbursement of PD, but not HD, has permitted to increase the use of PD over HD in many Asian countries like Hong Kong, Vietnam, Taiwan, Thailand, as well as in New Zealand and Australia over recent years [42, 43]. The major reasons of under utilization of PD modality include (1) lack or inadequate pre-dialysis education [44] and patient’s awareness of RRT options [7, 44, 45], and in particular the suitability and advantages of PD modality, (2) insufficient or lack of focus on patients’ training and encouragement and support, especially for anxious and unwell patients who might be nervous about participating in their own treatment [46-48], (3) lack or inadequate training of nursing staff and nephrologists in PD therapy [45, 49], (4) insufficient encouragement and support of medical and nursing staff to guide patients to chose or implement PD modality as a possible first choice therapy [45, 50], (5) lack or insufficient appreciation of the concept of “integrated renal replacement therapy (RRT) program” [1], and (6) inadequate preparation or lack of a proper set up of an independent PD unit [51, 52].
The success and continuity of a PD program relies on different factors including (1) enthusiasm and commitment of the PD team [53, 54], (2) continuous training program for medical and nursing staff, (3) structured educational program for predialysis chronic kidney disease (CKD) patients,(4) application of continuously updated policies and procedures, (5) and continuous evaluation and assessment of the applied program (table 3). Actually, implementation of these major steps should not only lay the foundation for solid PD program, but also should help in providing and maintaining adequate and unified standard technical PD performance [55] and successful continuity of the program (table 4).This approach should be reflected on extended patient’s PD treatment years, as an initial option of RRT, preservation of residual renal function, better preparation of kidney transplantation, delaying or avoidance of HD with vascular access problems, enjoying social life and more freedom together with least technical, infectious and non-infectious complications.
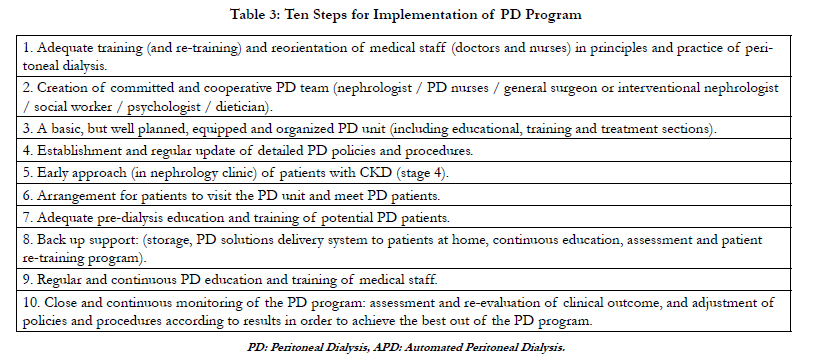
Table 3: Ten Steps for Implementation of PD Program
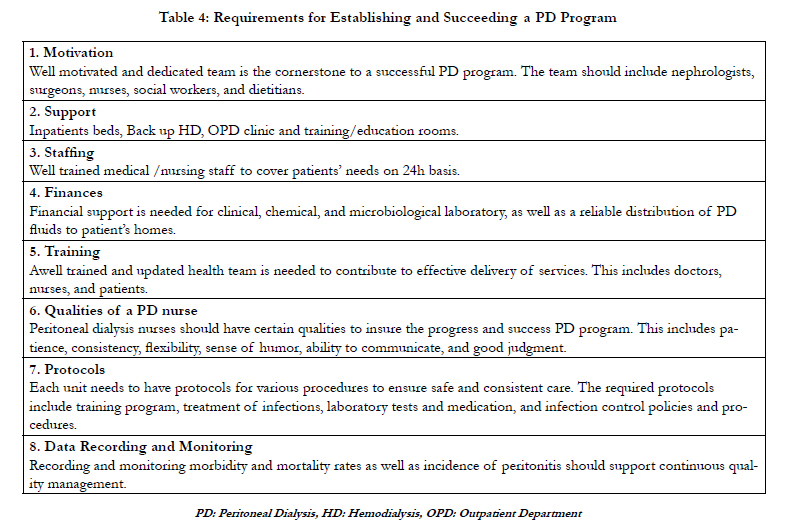
Table 4: Requirements for Establishing and Succeeding a PD Program
In conclusion, peritoneal dialysis constitutes an essential partof the integrated renal replacement therapy care for patients with ESRD. Despite the multiple benefits and advantages and improved technology in PD sets, solutions and cyclers, there hasn’t been much progress in PD utilization in many countries. The achievement and maintenance of a successful performance of PD unit requires the understanding and implementation of an integrated PD program concept, and the availability of essential needs and requirements. A structured model of PD program should be based on adequate theoretical and practical training of medical and nursing staff, and provides education and practical training of pre-dialysis ESRD patients and those transferred to PD from failed HD treatment. The program should be supported by detailed written and applied PD policies and procedures, including protocols for training and treatment of infections. The establishment of a purpose built, or transformed PD unit, together with continuous evaluation and assessment of performance can ensure the success and continuity. These measures, and the availability of trained and dedicated PD team, and the effectiveness of a training center in unifying the training standards and technique survival in support of PD program, should result in a successful performance and continuity of a PD program.
References
- Lameire N, Van Biesen W, Vanholder R (2000) The role of peritoneal dialysis as first modality in an integrative approach to patients with end-stage renal disease. Perit Dial Int. 20 (l): S134-S141.
- Karkar A, Abdelrahman MR (2011) Outcome of Patients Treated with Automated Peritoneal Dialysis: Effects of Selection of Patients. Saudi J Kidney Dis Transplant. 22(1): 40-48.
- McDonald SP, Marshall MR, Johnson DW, Polkinghorne KR (2009) Relationship between dialysis modality and mortality. J Am SocNephrol. 20(1): 155-163.
- Heaf JG, Lokkegaard H, Madsen M (2002) Initial survival advantage of peritoneal dialysis relative to haemodialysis. Nephrol Dial Transplant. 17(1): 112-117.
- Venosh EF, Snyder JJ, Foley RN, Collins AJ (2006) Mortality studies comparing peritoneal dialysis and hemodialysis: what do they tell us? Kidney Int. 103: S3-S11.
- Liem YS, Wong JB, Hunink MG, de Charro Fort, Winkelmayer WC (2007) Comarison of hemodialysis and peritoneal dialysis survival in the Netherlands. Kidney Int. 71(2):153-158.
- Mehrotra R, Devuyst O, Davies SJ, Johnso DW (2016) The Current State of Peritoneal Dialysis. J Am SocNephrol.
- Wang AYM (2007) The heart of peritoneal dialysis: residual renal function. Perit Dial Int. 27(2): 116-124.
- Franco MG, Lima G. (2007) Peritoneal dialysis in the elderly patients. Perit Dial Int. 27(3): S15.
- Brown EA (2008) Peritoneal dialysis for older people: Overcoming the barriers. Kidney Int. (108): S68-S71.
- Pereira B, Levey A (1997) Hepatitis C virus infection in dialysis and renal transplantation. Kidney Int. 51(4): 981-999.
- Cendoroglo M, Draibe S, Silva A, et al., (1995) Incidence and risk factors for hepatitis B virus and hepatitis C virus infection among hemodialysis and CAPD patients: evidence for environmental transmission. Nephrol Dial Transplant. 10(2): 240-246.
- Dombros N, Dratwa M, Feriani M, et al., (2005) European best practice guidelines for peritoneal dialysis. 5 Peritoneal dialysis solutions. Nephrol Dial Transplant. 20( 9): ix16-ix20.
- Frampton JE, Plosker GL (2003) Icodextrin: a review of its use in peritoneal dialysis. Drugs. 63(19): 2079-2105.
- Kim S, Oh J, Kim S, Chung W, Ahn C, Kim SG, Oh KH (2009) Benefits of biocompatible PD fluid for preservation of residual renal function in incident CAPD patients: a 1-year study. Nephrol Dial Transplant. 24(9): 2899-908.
- Youmbissi TJ, Malik TQ, Abdulrahman MR, Karkar A (2001) Simplified surgical placement of Tenckhoff catheter under local anesthesia: The Dammam Central Hospital experience. Saudi J Kidney Dis Transplant. 12 (2): 175-178.
- Little J, Irwin A, Marshall T, Rayner H, Smith S (2001) Predicting a patient’s choice of dialysis modality: experience in a United Kingdom renal department. Am J Kidney Dis. 37(5): 981-986.
- Jager KJ, Korevaar JC, Dekker FW, Krediet RT, Boeschoten EW (2004) The effect of contraindications and patient preference on dialysis modality selection in ESRD patients in The Netherlands. Netherlands Cooperative Study on the Adequacy of Dialysis (NECOSAD) Study Group. Am J Kidney Dis.43(5): 891-899.
- Rodd K, Wuerth D, Finkelstein FO (2006) Progress and Barriers that Continue to Challenge the CKD Educational Process. Perit Dial Int. 26 ( 1): 46A.
- Goovaerts T, Jadoul M, Goffin E (2005) Influence of a Pre-Dialysis Education Programme (PDEP) on the mode of renal replacement therapy. Nephrol Dial Transpl. 20(9): 1842-1847.
- Rubin HR, Fink NE, Plantinga LC (2004) Patient ratings of dialysis care with peritoneal dialysis vs. Hemodialysis. JAMA. 291(6): 697-704.
- Juergensen E, Wuerth D, Juergensen PJ (2006) Hemodialysis and peritoneal dialysis: patient’s assessment of their satisfaction with therapy and the impact of the therapy on their lives. Clin J Am SocNephrol. 1(6): 1191-1196.
- Flanigan MJ, Rocco MV, Prowant B (2001) Clinical performance measures: the changing status of peritoneal dialysis. Kidney Int. 60(6): 2377-2384.
- Badve SV, Hawley CM, Mcdonald SP, Mudge DW, Rosman JB, Brown FG, Johnson DW (2008) Automated and continuous ambulatory peritoneal dialysis have similar outcomes. Kidney Int. 73(4): 480-488.
- Ramos Sanchez A, Madonia C, Rascon-Pacheco RA (2008) Improved patient/ technique survival and peritonitis rates in patients treated with automated peritoneal dialysis when compared to continuous ambulatory peritoneal dialysis in a Mexican PD center. Kidney Int. 108: S76-S80.
- Venkataraman V, Nolph KD (2002) Utilization of PD modalities: evolution. Semin Dial. 15(6): 380-384.
- Keshaviah P, Emerson PF, Vonesh EF, Brandes JC (1994) Relationship between body size, fill volume, and mass transfer area coefficient in peritoneal dialysis. J Am SocNephrol. 4(10): 1820-1826.
- Michels MW, Verduijn M, Boeschoten EW, Dekker FW, KredietRT, (2009) Similar survival on automated peritoneal dialysis and continuous ambulatory peritoneal dialysis in a large prospective cohort. Clin J Am SocNephrol.4(5): 943-949.
- Huang JW, Hung KY, Yen CJ, et al., (2001) Comparison of infectious complications in peritoneal dialysis patients using either a twin-bag system or automated peritoneal dialysis. Nephrol Dial Transplant. 16(3): 604-607.
- Grothe C, Taminato M, Belasco A, Sesso R, Barbosa D (2016) Prophylactic treatment of chronic renal disease in patients undergoing peritoneal dialysis and colonized by Staphylococcus aureus: a systematic review and metaanalysis. BMC Nephrology. 17(1): 115.
- Davison SN, Jhangri GS, Jindal K, Pannu N (2009) Comparison of volume overload with cycler-assisted versus continuous ambulatory peritoneal dialysis. Clin J Am SocNephrol. 4(6): 1044-1050.
- Mujais S, Nolph K, Gokal R, et al., (2000) Evaluation and management of ultrafiltration problems in peritoneal dialysis. International Society of peritoneal Dialysis Ad Hoc Committee on Ultrafiltration Management in Peritoneal Dialysis. Perit Dial Int. 20(4): S5-S21.
- Blake P (1999) Advantages and disadvantages of automated peritoneal dialysis compared to continuous ambulatory peritoneal dialysis. Perit Dial Int. 19(2): S121-S124.
- De Wit GA, Merkus MP, Krediet RT, et al., (2001) A comparison of quality of life of patients on automated and continuous ambulatory peritoneal dialysis. Perit Dial Int. 21(3): 306-312.
- Jain AK, Blake P, Cordy P, Garg AX (2012) Global trends of peritoneal dialysis. J Am SocNephrol. 23(3): 533-544.
- Brown EA, Davies SJ, Heimburger O, et al., (2001) Adequacy targets can be met in anuric patients by automated peritoneal dialysis: baseline data from the EAPOS. Perit Dial Int. 21 (13) : S133-S137.
- Lameire N, Peeters P, Vanholder R, Van Biesen W (2006) Peritoneal dialysis in Europe: an analysis of its rise and fall. Blood Purif. 24(1): 107-114.
- Struijk DG (2015) Peritoneal Dialysis in Western Countries. Kidney Dis. 1(3): 157-164.
- Remón-Rodríguez C, Quirós-Ganga P, Portolés-Pérez J, Gómez-Roldán C, Miguel-Carrasco A, et al., (2014) GrupoCooperativoRegistrosEspañoles de Diálisis Peritoneal [Results of the cooperative study of Spanish peritoneal dialysis registries: analysis of 12 years of follow-up]. Nefrologia. 34(1): 18-33.
- MacNeill SJ, Casula A, Shaw C, Castledine C (2016) UK Renal Registry 18th Annual Report: Chapter 2 UK Renal Replacement Therapy Prevalence in 2014: National and Centre-specific Analyses. Nephron. 132(1): 41-68.
- Najafi I (2009) Peritoneal dialysis in iran and the middle East. Perit Dial Int. 29 (2): S217-S221.
- USRDS Annual Data Report (2014) Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. Am J Kidney Dis. 63(1): e1-e478.
- Kwong VW, Li PK (2015) Peritoneal dialysis in Asia. Kidney Dis. 1(3): 147- 156.
- Karkar A (2011) The value of pre-dialysis care. Saudi J Kidney Dis Transplant. 22 (3): 419-427.
- Karkar A (2011) Caring for patients with chronic kidney disease: benefits and rewards. Int J Nephrol. 11(40): 6.
- Bernardini J, Price V, Figueiredo A (2006) Peritoneal dialysis patient training, (ISPD guidelines/recommendations). Perit Dial Int. 26: 625-632.
- Swiech-Bruce C (2009) Training tool empowers elderly. Perit Dial Int. 29 (1): S5-S15.
- Kazancioglu R, Ozturk S, Yucel L, Guvenc S, Ekiz S, Dogan S (2008) Importance of home visits in peritoneal dialysis. Dialysis & Transplantation. 37(4): 132-136.
- Troidle LK, Kliger AS, Finkelstein FO (2006) Barriers to CPD utilization in network#1, New England. Perit Dial Int. 26(4): 452-457.
- Durand PY and Verger C (2006) The state of peritoneal dialysis in France. Perit Dial Int. 26: 654-657.
- Finkelstein FO (2006) Structural requirements for a successful chronic peritoneal dialysis program. Kidney Int. (103): S118-21.
- Mehrotra R, Khawar O, Duong U, Fried L, Norris K, Nissenson A, Kalantar- Zadeh K (2009) Ownership patterns of dialysis units and peritoneal dialysis in the United States: utilization and outcomes. Am J Kidney Dis. 54(2): 289-98.
- Diaz-Buxo JA, Crawford-Bonadio TL, St. Pierre D, Ingram KM (2006) Establishing a successful home dialysis program. Blood Purif. 24(1): 22-27.
- Piraino B.(2006) Nurses and physicians working together. Perit Dial Int. 26(6): 641-642.
- Youmbissi TJ, Malik TQ, Rafi A, Al Ahmad F, Sinha AK, Abdulrahman M, Karkar A (2001) CAPD in Dammam Central Hospital, Saudi Arabia: A fiveyear experience. Saudi J Kidney Dis Transplant. 12 (4): 511-515.





