Visual Hallucinations: Identifying Charles Bonnet Syndrome
Pang L
Western University of Health Sciences, College of Optometry, 309 E. Second St., Pomona, CA 91766, USA.
*Corresponding Author
Linda Pang, OD, FAAO,
Western University of Health Sciences, College of Optometry, 309 E.
Second St., Pomona, CA 91766, USA.
E-mail: LPANG@WESTERNU.EDU
Article Type: Short Description
Received: November 06, 2015; Accepted: January 29, 2015; Published: February10, 2015.
Citation: Pang L (2015) Visual Hallucinations: Identifying Charles Bonnet Syndrome. Int J Ophthalmol Eye Res. S1:004, 14-22. doi: dx.doi.org/10.19070/2332-290X-SI01004.
Copyright: Pang L© 2015. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Charles Bonnet Syndrome (CBS) is a rare condition comprised of visual hallucinations, which occur in the context of damage anywhere along the visual pathway and absence of hallucinations affecting other sensory modalities. Patients with CBS maintain partial or full insight that the hallucinations are not real, have no psychological conditions, and maintain intellectual functioning. CBS has been well documented in the neurologic, geriatric medicine, and psychiatric literature, but there is a lack of information in the optometric/ophthalmologic literature. Therefore, increased awareness of the signs and symptoms associated with CBS is required among eye care professionals. To better understand why visual hallucinations occur, the neurobiology underlying visual hallucinations will be discussed. This article will also explain etiologies of visual hallucinations, the pathophysiology of CBS, as well as effective management strategies.
2.Introduction
3.History
4.Prevalence
5.Definitions
6.Characteristics of Charles Bonnet Syndrome
6.1 CBS and Visual Acuity
7.Etiologies of Visual Hallucinations
7.1 Neurologic Disorders Known to Cause Visual Hallucinations
7.2 Prescription medications may induce visual hallucinations
7.3 Illicit drugs may induce visual hallucinations
7.4 Psychiatric disorders may be accompanied by visual hallucinations
8.Pathophysiology of Charles Bonnet Syndrome
8.1 Deafferentation Theory
9.Visual Pathways
10.Neurobiology of visual hallucinations
11.Management Strategies
11.1 Optical intervention
11.2 Surgical intervention
11.3 Multi-disciplinary approach
11.4 Medical Therapy
11.5 Patient Education
12.Conclusion
13.References
Keywords
Visual Hallucinations; Visual Cortex; Charles Bonnet Syndrome.
Introduction
Visual hallucinations experienced by patients are not uncommon and may occur with visual impairments, neurological diseases, psychiatric conditions, and use of certain medications. These visual hallucinations can be disturbing to those who experience them because of the negative connotation associated with hallucinations as a sign of mental instability. However, there is a condition, Charles Bonnet Syndrome (CBS), which includes visual hallucinations due to damage along the visual pathway in the absence of hallucinations affecting other sensory modalities [1]. Patients with CBS maintain partial or full insight that the hallucinations are not real, have no psychological conditions, and maintain intellectual functioning [1].
CBS has been documented well in the neurologic, geriatric medicine, and psychiatric literature. However, due to the lack of information in the optometric/ophthalmologic literature, increased awareness needs to be established among eye care professionals. Since visual hallucinations occur in the presence of vision loss or deprivation to the visual system, eye care professionals must recognize the symptoms of CBS to provide appropriate information and management to patients experiencing visual hallucinations associated with CBS.
History
In 1760, a Swiss scientist named Charles Bonnet, who was well known for his contributions to botany and philosophy, first described visual hallucinations associated with CBS. Bonnet documented the complex visual hallucinations experienced by his 90-year-old grandfather, Charles Lullin, and published his findings in an essay [1].
Ironically, Charles Bonnet suffered from an unknown cause of vision loss and experienced visual hallucinations. However, it was
not until 1967 that another Swiss scientist, George De Morsier, coined the term, “Charles Bonnet Syndrome”. De Morsier was
known well for his contributions in neuro-developmental disorders [1].
Prevalence
The prevalence of CBS varies and ranges from 0.4% up to 30%, depending on the study [1,3-6] Khan et al. [4] noted that the incidence of CBS was statistically higher in subjects with worse visual acuity. This finding demonstrated that worse vision is associated to some degree with increased risk of experiencing visual hallucinations [4].
There are several reasons, which explain the variability in the prevalence rates of CBS. Firstly, there is no universal definition of CBS agreed upon by all healthcare professionals. Secondly, the diagnosis of CBS is made across different disciplines, including: optometry, ophthalmology, geriatric medicine, psychiatry, and neurology. Thirdly, many people are hesitant to report that they are experiencing visual hallucinations for fear of being labeled as mentally unstable [1,7-9] As the geriatric population increases, the amount of acquired vision loss will also increase. As a result, there will be an increase in those affected by CBS. As health care providers, we need to understand and recognize this condition so these individuals can be properly managed. In a study by Gilmour et al, only 9% of people experiencing CBS sought medical advice. Disappointingly, only half of them received an explanation about CBS [35].
Definitions
There are various definitions that have been used to classify CBS, but there has been no consensus on which definition is most accurate. Gold and Rabins’ definition [10] (1989) is most commonly used in the psychiatric literature. They describe the visual hallucinations in CBS to be stereotyped, formed, complex, persistent or repetitive in nature [10]. Further, they suggest that those with CBS are aware that the hallucinations are not real. Also, with Gold and Rabins’ definition, there are no delusions or hallucinations affecting other sensory modalities. In this definition, ocular pathology is not part of the diagnostic criteria [10].
Ophthalmologists and neurologists use CBS to describe visual hallucinations that occur as a result of ocular pathology or visual pathway disease. The type of hallucinations and age of the patient are of secondary importance [12]. The definition used by ophthalmologists and neurologists supports Bonnet’s original description of the condition. An important consideration about the ophthalmologically-defined CBS is that it carries an inherent ambiguity: Was the ocular pathology or the loss of acuity the contributing factor for the visual hallucinations .
Characteristics of Charles Bonnet Syndrome
Visual hallucinations experienced by CBS patients are typically simple or complex in nature, but a full spectrum of hallucinations can occur. Simple visual hallucinations, which are sometimes described as elementary or formed, are composed of photopsias, simple shapes, grid-like patterns, and branching patterns. Complex visual hallucinations are made up of vivid and complicated images of people, faces, vehicles, animals, flowers, trees, plants, and miniature images of people and objects [7].
The visual hallucination episodes last seconds to a few hours, with recurrent episodes of visual hallucinations occurring for days to years. A majority of the visual hallucinations are strange or bizarre to the patients, but they are seldom disturbing. Generally, people experiencing visual hallucinations remain neutral about the hallucinations [1].
Complex visual hallucinations are emphasized in the CBS definitions. However, CBS patients experience simple visual hallucinations most frequently. Even though these patients have some level of visual impairment, the visual hallucinations are in more detail and better clarity than their residual vision. These visual hallucinations are vivid images such as that seen in normal viewing conditions and are not under voluntary control [13,32].
BS hallucinations are purely visual in nature and do not involve hallucinations in other sensory modalities [14,36]. Further, CBS visual hallucinations occur in a clear state of consciousness when the patient is alert and awake. These patients show no signs of dementia and maintain preserved intellectual functioning, including: mental awareness, perception, reasoning, judgment, processing information, and ability to apply knowledge [14]. People experiencing the hallucinations maintain insight that the hallucinations are not real.
Madill et al. studied the occurrence of CBS in 4 patients with advanced glaucoma [12]. They challenged previous authors who stated that acuity loss is required for ophthalmologically-defined CBS. In these advanced glaucoma patients, visual acuity ranged from 20/20 to 20/40 monocularly with extensive visual field defects. No hallucinations occurred in other sensory modalities, and all maintained insight that the hallucinations were not real. The results of Madill et al.’s case study coincide with the ophthalmological definition of CBS, where it emphasizes ocular pathology or visual pathway disease as a cause of the visual hallucinations. It is important to understand this case series emphasizes that visual acuity loss is not a requirement for CBS visual hallucinations to occur [12].
With that said, an association between age-related macular degeneration (ARMD) and colored visual hallucinations has been proposed. Signals related to color vision pass through the parvocellular layers of the lateral genicular nucleus (LGN) and are
transmitted along the ventral color pathway. In patients with macular degeneration, there is degeneration throughout the ventral color pathway [15]. Damage to the cone photoreceptors in the macula creates a lack of visual input to the color areas of the visual association cortex. Because of the reduced visual input to the visual association cortex, endogenous activation within the color area results in colored hallucinations. Functional magnetic resonance imaging (fMRI) provides support for this theory, as the color area of the visual association cortex remained hyperactive in CBS patients with macular degeneration [15].
Because of the physiological deafferentation with ganglion cell loss in glaucoma, they can experience CBS without an acuity loss. Whereas in ARMD, there is loss of central retinal ganglion cells, which causes CBS to occur with an acuity loss [12]. Therefore, patients with significant ocular disease and preserved visual acuity may still be at risk for developing CBS
Etiologies of Visual Hallucinations
Determining the etiology responsible for the visual hallucinations is required to implement the appropriate management. Table 1 outlines a sampling of the common etiologies of visual hallucinations.
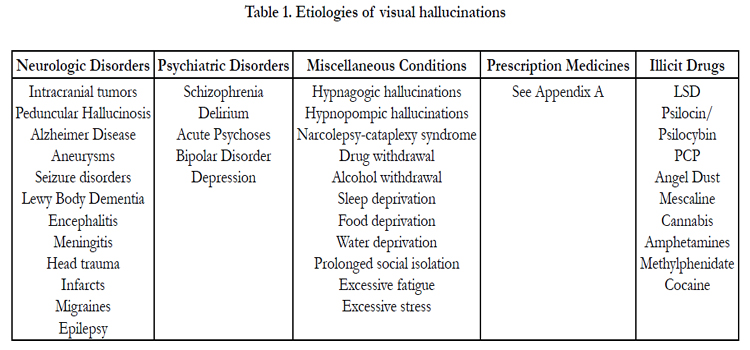

Table 1. Etiologies of visual hallucinations
In Parkinson’s Disease, there are defects in the visual pathway associated with the dopamine deficiency in the retina and central pathways. Levodopa increases the dopamine levels, which should also improve the visual system’s function [16]. Their visual hallucinations are attributed to the decreased vision, cognitive impairment, dopaminergic medications, or anticholinergic medications [17].
According to Manford and Andermann [16] in 1998, visual hallucinations were not reported until after Parkinson’s disease treatment was initiated such as anticholinergics, Levodopa, and dopaminergic agonists [16]. Parkinson’s disease patients maintain insight that the hallucinations are not real.
Peduncular hallucinosis shows the closest clinical overlap with CBS [18]. The underlying etiology of peduncular hallucinosis is vascular in nature. Complex visual hallucinations occur as a result of lesions in the midbrain and/or thalamus. The term “peduncular” does not only imply the cerebral peduncles, but it includes the midbrain and the surrounding area. Peduncular hallucinosis has been associated with other central nervous system (CNS) pathologies, including: vascular and infectious pontine, midbrain, and thalamic lesions, local subarachnoid hemorrhage, compression by local and distal tumors, basilar vascular hypoplasia, basilar migraine, and after surgical and angiographic interventions [18]. The common hallucinations experienced by these patients include people, animals, landscapes, grotesque and deformed faces, repeated patterns, and Lilliputian hallucinations. Lilliputian hallucinations are visual phenomena in which the hallucinations are miniature in size.
Peduncular hallucinosis typically occurs a few days after the infarct. Each hallucination episode will last for a few minutes to several hours and can be accompanied by tactile or auditory hallucinations differentiating it from CBS. Patients with peduncular hallucinosis may continue to experience episodes of hallucinations for several weeks up to years. These patients maintain insight that the hallucinations are not real [16]. Treating the underlying CNS pathologies will resolve the hallucinations. Therefore, it is important to screen radiologically for CNS disease to rule out peduncular hallucinosis from CBS.
A study evaluated the regional cerebral blood flow (rCBF) using brain Single Photon Emission Computed Tomography (SPECT) in patients experiencing CBS visual hallucinations [19]. There was an increased perfusion in rCBF in the regions of the lateral temporal cortex, striatum, and thalamus in patients who experienced visual hallucinations. This suggests that, when people have vision loss, increased cortical activation in the areas of the lateral temporal cortex, striatum, and thalamus contribute to the development of visual hallucinations [19,32,36].
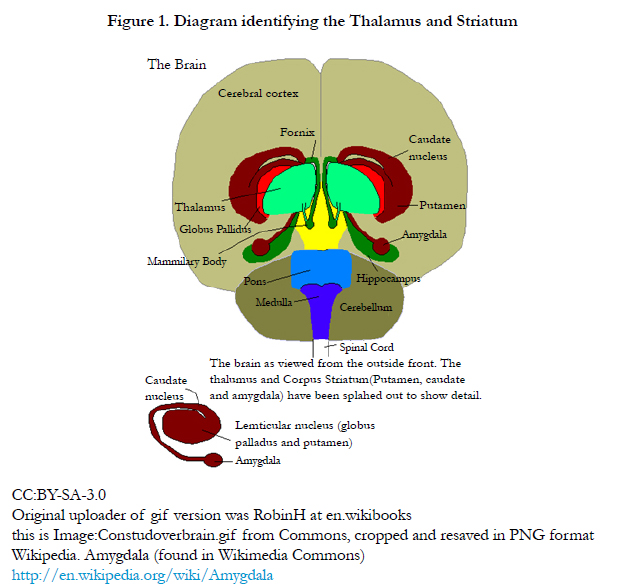
Figure 1. Diagram identifying the Thalamus and Striatum
CC:BY-SA-3.0
Original uploader of gif version was RobinH at en.wikibooks
this is Image:Constudoverbrain.gif from Commons, cropped and resaved in PNG format
Wikipedia. Amygdala (found in Wikimedia Commons)
en.wikipedia.org/wiki/Amygdala
Prescription medications can have a side effect of visual hallucinations by mechanisms that are unknown [16,20,21]. Appendix A includes a comprehensive list of these medications [20,21]. Alpha-2 agonists such as Brimonidine Tartrate have been shown to cause systemic and neuropsychiatric phenomena and may induce CBS [22]. Because it is a well-known lipophilic agent, it has the ability to penetrate the blood-brain barrier and cause systemic side effects such as visual and auditory hallucinations, depression, confusion, and anxiety in adults [23,31]. In children, it can cause adverse effects which include coma, hypotension, bradycardia, hypotony and hypothermia [31]. The study by Tomsak et al. [22] reported that their four primary open angle glaucoma subjects experienced visual hallucinations within 5 days to 2.5 months after starting Brimonidine Tartrate therapy [22]. The authors found that the visual hallucinations resolved after the discontinuation of Brimonidine Tartrate [22]. A case report by Garcia-Catalan et al describes an 81-year old female with pseudoexfoliation glaucoma and age-related macular degeneration developed visual hallucinations after 1 month of using Brimonidine with complete resolution of the hallucinations upon suspending its use [31]. However, It was Rahman et al. [23] who concluded that the visual hallucinations are a rare side effect of the medication [23].
Mescaline and Lysergic Acid Diethylamine Tartrate (LSD) are hallucinogens which act on specific serotonin (5-hydroxytryptamine: 5HT2) receptors. LSD is active on serotonergic neurons. With these hallucinogens, insight is maintained, and there is no evidence of psychosis or delusions. The visual hallucinations experience can be visual distortions, colored patterns, shapes, figures of people and animals, have distortions in size, and involve feelings of fantasy [16].
Stimulants, such as amphetamine and cocaine, more commonly cause auditory or tactile hallucinations. Cocaine acts on specific
serotonin (5HT3) receptors, dopamine receptors, and catecholamine receptors, which are all concentrated in the limbic system.
They may begin as simple hallucinations and later develop into vividly-colored, complex hallucinations. They are more easily seen with the eyes closed or in the dark [16].
Visual hallucinations may be prominent in people with psychoses. However, those with psychosis will also have hallucinations affecting other sensory modalities, which differentiates it from CBS [20]. There are many studies, which evaluate whether isolated visual hallucinations may be a precursor for developing dementia. [14,24,25] In Guerra-Garcia’s study (1997) [25], CBS patients underwent a specific imaging test called the brain SPECT [25]. SPECT revealed reduced perfusion in the mid-parietal area and occipital areas. The hypoperfusion in the parietal area closely corresponds to the SPECT pattern, which exists in Alzheimer’s disease and other forms of dementias.
In a study of patients with ARMD, Holroyd and Rabins [11] (1996) found that the slightly lower cognitive scores for subjects who experienced visual hallucinations compared to cognitive scores of patients without hallucinations were not statistically significant [11]. Isolated visual hallucinations were not an early symptom of progressive dementia in this study. The relationship between visual hallucinations and the development of dementia is still uncertain.
In schizophrenia, visual hallucinations occur more commonly than thought previously. It occurs typically with a delusional component that is not normally seen in organic causes. As schizophrenia progresses, the clarity of the hallucinations may deteriorate, which is distinct from CBS [16]. Table 2 outlines the other clinical characteristics, which are useful in differentiating schizophrenia-related visual hallucinations from organic disease related visual hallucinations.
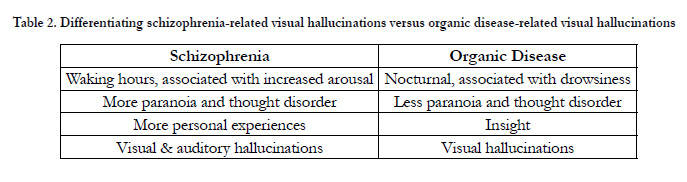
Table 2. Differentiating schizophrenia-related visual hallucinations versus organic disease-related visual hallucinations
Pathophysiology of Charles Bonnet Syndrome
Pathophysiology of Charles Bonnet Syndrome The true underlying mechanism in the formation of visual hallucinations associated with CBS is not exactly known [1,3,4,20,26] There are a few theories, which have been well-recognized and are used to explain CBS. Hallucinations can result from a release by the visual association cortex, acting by loss of cortico-cortical inputs, and alteration of serotonergic processes [16].
The deafferentation theory is the hypothesis, which is accepted most commonly to explain CBS. Deafferentation means the loss of visual input into the brain, which will lead to a change in the excitability of the visual association cortex [12]. When the sensory visual input into the cortex is removed, such as with ocular pathology or damage to the visual pathway, spontaneous neuronal discharge in the visual association cortex occurs, increasing the excitability within the visual association cortex. As a result, visual hallucinations will be released [1,19,36].
The increase in excitability in the visual association cortex occurs for a variety of reasons:
1. an increase in the number of neurotransmitters released in the presynaptic neuron caused by presence of increased vesicles.
2. an increase in the number of receptors in the postsynaptic membrane caused by prolonged inactivity which also leads to
an increase in the intensity of the response.
3. changes in the amount of gamma-aminobutyric acid and glutamatergic N-Methyl-D-aspartic acid within the synapse
has been shown to contribute to the hyperexcitability of the neurons [32].
Since the visual system has plasticity, it can lead to sprouting new axons in the damaged area and reorganization of the receptive fields. Therefore, small amounts of remaining stimulus from the retina, optic tract, or other structures within the visual system can elicit a visual hallucination because the neurons are more sensitive [32].
Phantom sensations, such as auditory hallucinations, in the recently deaf or phantom tactile sensations in amputees represent
similar phenomenon as CBS, except in different sensory domains. Due to the absence of afferent sensory input to the brain, when
sensory input in decreased, the CNS increases activity. This increased activity is interpreted as hallucinations in the corresponding sensory system [20].
Visual Pathways
After visual information leaves the LGN, it passes along the optic radiations and is finally transmitted to the primary visual cortex (Brodmann Area 17). From the primary visual cortex, it will transmit information to the secondary visual cortex (Brodmann Area 18) and finally transfer the visual information to the higher processing areas of the visual association cortices (Brodmann Area 19, 37) [19].
The primary visual cortex (Brodmann Area 17) is responsible for simple visual hallucinations. The secondary visual cortex (Brodmann Area 18) and visual association cortices (Brodmann Area 19, 37) are accountable for complex visual hallucinations 2,13].
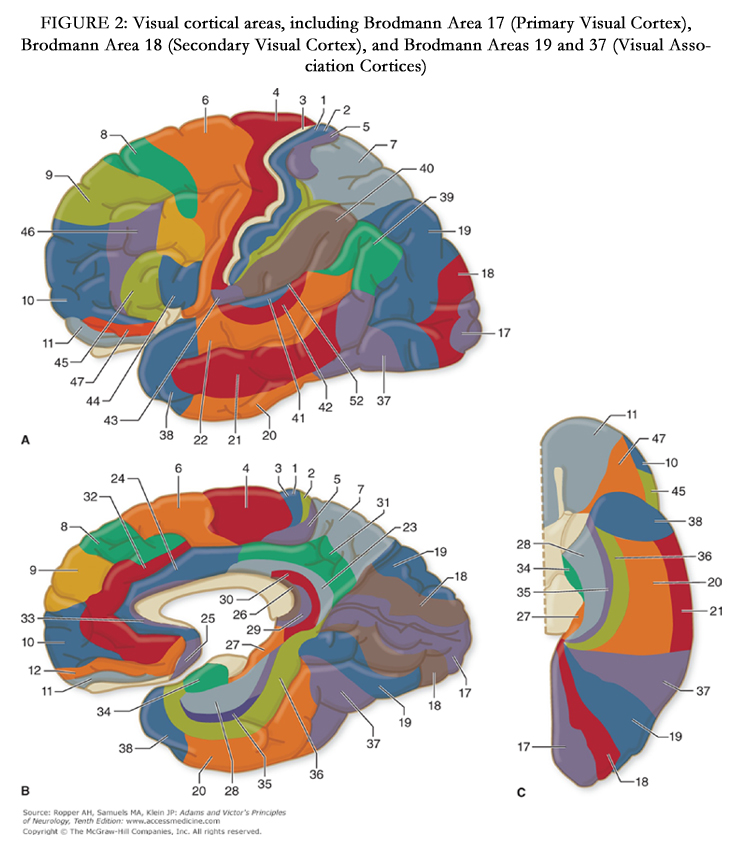

Figure 2. Visual cortical areas, including Brodmann Area 17 (Primary Visual Cortex), Brodmann Area 18 (Secondary Visual Cortex), and Brodmann Areas 19 and 37 (Visual Association Cortices)
Source: Ropper AH, Samuels MA, Klein JP: Adams and Victor's Principles of Neurology, Tenth edition: www.accessmedicine.com
Copyright © The McGraw-Hill Companies, Inc, All rights reserved.
From: Chapter 22. Neurologic Disorders Caused by Lesions in Specific Parts of the Cerebrum. Adams and Victor's Principles of Neurology, 10e, 2014
Legend: Cytoarchitectural zones of the human cerebral cortex according to Brodmann. A. Lateral surface. B. Medial surface. C. Basal inferior surface. The functional zones of the cortex are illustrated in Fig. 22-3.
Neurobiology of visual hallucinations
An understanding of the underlying functional neurobiology will help to understand the areas of the visual cortex, which are
responsible for stimulating specific visual hallucinations. Neuroimaging studies are providing insight into the science of visual hallucinations. Functional MRI studies have been conducted on patients experiencing visual hallucinations. In these studies, the fMRI is used to identify the cerebral location relating to the visual hallucinations. Santhouse et al. [15] (2000) found that visual hallucinations were related to increases in activity within specialized areas of the visual association cortex [15].
Functional MRI studies revealed that when visual hallucinations occur, the occipital cortex has a decreased response to external visual stimuli. The decreased response to sensory input allows endogenous visual stimuli to be perceived as hallucinations [2].
There is a relationship between the content of the hallucinations and the corresponding regions within the ventral occipital lobe. The ventral occipito-temporal cortex, also known as the ventral occipital lobe, is highly specialized for complex visual hallucinations, such as: landscapes, figures, faces, people, vehicles, trees, shrubs, and Lilliputian hallucinations [10,13,32,36].
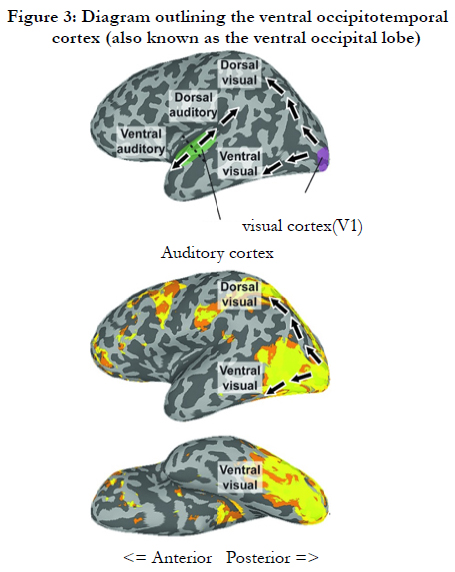

Figure 3: Diagram outlining the ventral occipitotemporal cortex (also known as the ventral occipital lobe)
Caption
Fig 3: Dorsal and ventral visual and auditory cortical pathways. (a) Illustration of the dorsal and ventral visual and auditory cortical pathways. Black dotted line shows the distinction between anterior and posterior parts of the auditory cortex. (b) Positive activation elicited by viewing movies of body parts relative to a fixation baseline (unthresholded) with the schematic pathways overlaid. Two streams of activation are clearly visible, one extending into the superior parietal cortex and other onto the lateral and ventral surfaces of occipitotemporal cortex (With thanks to A. Chan)
Book: MRI in Psychiatry. Authors. Harel, Assaf; Baker, Chris I.
Book: MRI in Psychiatry
The amount of cortical tissue available in the corresponding region has been suggested as being responsible for why certain simple or complex hallucinations occur more frequently than others [7]. The greater the amount of cortical tissue, the more frequently it will be endogenously activated [7].
The ventral occipital lobe lies closely to the amygdala, which is responsible for the emotional response to hallucinations [15]. In a study by Santhouse et al. [15], they conducted a questionnaire regarding variables associated with visual hallucinations. [15] Half of the 34 CBS patients did not notice an emotional connection to their hallucinations. Of the patients who did have an emotional connection to the hallucinations, only half of them found the hallucinations to be unpleasant [15].
The areas shown in Table 3 and Figure 4 reveal the location within the ventral occipital lobe that correspond to the type of visual hallucination experienced.
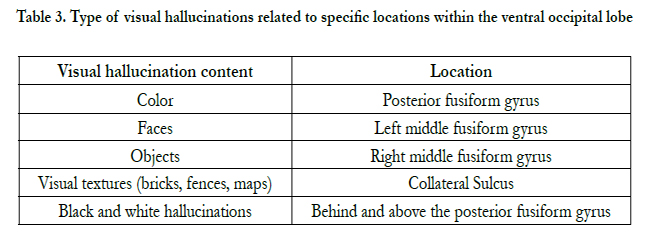
Table 3. Type of visual hallucinations related to specific locations within the ventral occipital lobe
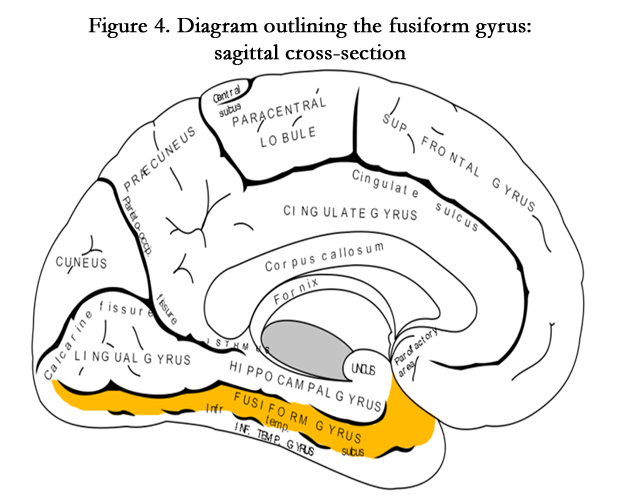
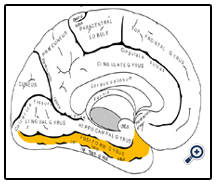
Figure 4. Diagram outlining the fusiform gyrus: sagittal cross-section
By Gray, vectorized by Mysid, colourd by was_a_bee. (File:Gray727.svg) [Public domain], via Wikimedia Commons
commons.wikimedia.org/wiki/File%3AGray727_fusiform_gyrus.png
Management Strategies
In the management of these patients, it is important to remember that CBS is a diagnosis of exclusion. Other etiologies that
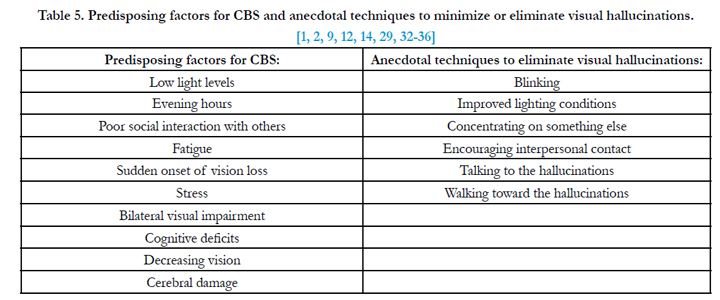
can cause visual hallucinations must be investigated and ruled out before concluding that it is CBS [1]. CBS may be difficult to discriminate among other co-morbidities. However, asking the necessary questions (see Table 4), as well as understanding the predisposing factors of and anecdotal means of alleviating visual hallucinations (see Table 5), aids in the differential diagnosis. Patients meeting the requisite criteria are then managed for their visual hallucinations using:
1. low vision rehabilitation including optical intervention (spectacles, contact lenses, and optical aids)
2. surgical intervention,
3. multi-disciplinary approach,
4. medical therapy, and
5. patient education.
It is necessary to refer patients who meet the following criteria:
1. are experiencing other neurological symptoms,
2. have hallucinations affecting other sensory modalities,
3. have insight that the visual hallucinations are real, or
4. have visual hallucinations that did not occur after vision loss.
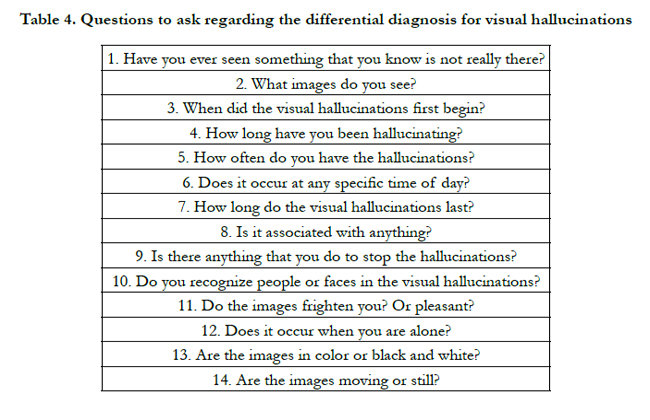
Table 4. Questions to ask regarding the differential diagnosis for visual hallucinations
The first step in managing these patients with visual hallucinations is to maximize their remaining vision as much as possible either through spectacles, contact lenses, optical aids, or low vision rehabilitation. By improving the vision, it is possible to reduce the frequency of the visual hallucinations [1,32-34].
In 2004, Eperjesi and Akbarali [8] found that visual hallucinations decreased in frequency when patients used optical devices [8]. In this study, the patients were prescribed ground-in prism, monocular telescope, best-corrected spectacles, tinted sunglasses, and nightlights. All of these interventions were effective in reducing or eliminating visual hallucinations for these patients. The reason why these interventions were successful in resolving visual hallucinations was because they provide the sharpest images possible to the retina by reducing blur, glare, and field loss. It is unlikely that the hallucinations resolved spontaneously because the visual hallucinations returned once the interventions were stopped [8].
If surgical intervention is appropriate, treating the underlying cause of the visual impairment can halt the visual hallucinations. Cataract extraction improved the vision and eliminated the visual hallucinations in a patient with bilateral cataracts. Laser intervention for the treatment of proliferative diabetic retinopathy also reduced visual hallucinations in a patient. Laser photocoagulation in a patient with subretinal hemorrhage reduced the occurrence of visual hallucinations [8,32].
In order to rule out pathological causes of visual hallucinations and to confirm intact cognition, utilizing a multi-disciplinary approach is beneficial. As an eye care professional, it is important to rule out other ocular causes of visual hallucinations such as photopsias caused by vitreo-retinal tractions or retinal detachments.
If a patient reports visual hallucinations, the primary care practitioner should rule out metabolic, infectious, toxic, and neurologic etiologies of the visual hallucinations. A physical and neurological examination, blood workup, and medication review are indicated [1,36].
Referral to a psychologist or psychiatrist may need to be made to confirm intact cognition with formal cognitive tests. Neuroimaging tests such as MRI or Computed Tomography (CT) may be indicated to aid in determining the cause of the visual hallucinations [1,36].
When optical or surgical interventions are ineffective, pharmacological therapy may be instituted if the visual hallucinations are distressing to the patient. Referring the patient to a psychiatrist for pharmacological management is appropriate if the hallucinations distress the patient.
Certain pharmacologic agents exacerbate or stimulate the development of visual hallucinations. Serotonin and acetylcholine are important neurotransmitters for the development of visual hallucinations. These neurotransmitters are concentrated in the visual thalamic nuclei and visual cortex, which are not found in other sensory modalities. This explains why CBS visual hallucinations do not affect hallucinations in other sensory modalities [16].
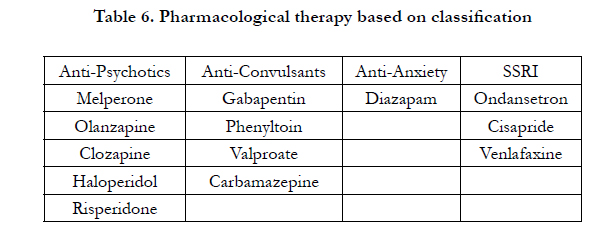
Table 6. Pharmacological therapy based on classification
Research has shown the sensory deprived cortex has significantly lower serotonin levels [27]. When there is an interruption in relaying visual information to the visual cortex due to ocular pathology or deprivation of the visual system, the serotonergic processes are reduced. As a result, endogenous excitatory signals are released in the visual association cortex. These excitatory signals become misinterpreted as visual hallucinations. The medications, which restore serotonin to the visual cortex, have been shown to be effective in reducing symptoms of visual hallucinations [27].
Antipsychotics, anticonvulsants, antianxiety, and SSRIs have been shown, albeit with inconsistent results, in the literature to reduce or eliminate visual hallucinations associated with CBS [8,26,28]. The studies that investigated the efficacy of these medications utilized small sample sizes and provided short term results [29]. It is difficult to determine whether the same results will transfer to a larger population of patients and whether the effects can be sustained for a long period of time (see Table 6, for a brief listing).
Currently there are no well-established medications for the treatment of CBS given the majority of reported cases that are documented in the literature are small case reports or case series therefore the results are not generalizable for all patients with CBS [33]. It is imperative to conduct more randomized clinical trials under age and gender-matched conditions to evaluate the side effects of the medications and how they will affect CBS patients [28]. Pharmacological treatment needs to be reserved only for those CBS patients, who are very distressed by the hallucinations because of the inconclusive results in effectivity [30,33].
One of the most important elements involved with managing CBS patients is properly educating the patients and their families about the condition.[8] Many elderly patients affected by CBS fear that the visual hallucinations are signs of dementia or mental instability. Educating and reassuring patients that the condition is benign and may be a common response after vision loss may help to relieve distress in those suffering from the condition 10,32-35].
Learning that CBS is unrelated to mental illness provides relief to patients and their families [8]. It is beneficial to inform patients that, while the visual hallucinations usually resolve spontaneously, they may persist in some cases [10,18].
These patients should be encouraged to join support groups to meet other individuals suffering from similar ocular pathologies who may be experiencing similar phenomena. They can discuss their experiences with others, provide reassurance to one another, and offer techniques for reducing the hallucinations [8].
Conclusion
Although awareness of CBS in the medical literature has increased over the past few decades, there remains a paucity of information about this rare condition in the optometric/ ophthalmologic literature. Criteria for diagnosing CBS include: visual hallucinations, absence of hallucinations in other sensory modalities, partial or full insight that hallucinations are not real, absence of psychological disorders, preserved intellectual functioning. There is no lower limit of Snellen visual acuity, and no specific age requirement.
Knowledge of CBS allows for proper diagnosis and appropriate management of the patients to reduce the visual hallucinations.
Recognizing the symptoms of CBS permits the healthcare professional to share appropriate information about the condition
with the patient and the family. This increased awareness about CBS among eye care professionals will benefit and insure the
effective management of patients with symptoms of visual hallucinations.
References
- Kester EM (2009) Charles Bonnet syndrome: Case presentation and literature review. Optometry 80(7):360-366.
- Menon GJ, Rahman I, Menon SJ, Dutton GN (2003) Complex Visual Hallucinations in the Visually Impaired: The Charles Bonnet Syndrome. Surv Ophthalmol 48(1):58-72.
- Rovner BW (2006) The Charles Bonnet syndrome: a review of recent research. Curr Opin Ophthalmol 17(3): 275-277.
- Khan JC, Shahid H, Thurlby DA, Yates JRW, Moore AT (2008) Charles Bonnet Syndrome in Age-Related Macular Degeneration: The Nature and Frequency of Images in Subjects with End-Stage Disease. Ophthalmic Epidemiol 15(3):202-208.
- Schultz G, Melzack R (1991) The Charles Bonnet syndrome: “phantom visual images.” Perception 20(6):809-825.
- Teunisse RJ, Zitman FG, Raes DCM (1994) Clinical Evaluation of 14 Patients With the Charles Bonnet Syndrome (Isolated Visual Hallucinations). Compr Psychiatry 35(1):70-75.
- Wilkinson F (2004) Auras and other hallucinations: windows on the visual brain. Prog. Brain Res. 144:305-320.
- Eperjesi F, Akbarali N (2004) Rehabilitation in Charles Bonnet syndrome: a review of treatment options. Clin Exp Optom 87(3): 149-152.
- Chen CS, Lin SF, Chong MY (2001) Charles Bonnet Syndrome and Multiple Sclerosis. Am J Psychiatry 158(7): 1158-1159.
- Ffytche DH (2007) Visual hallucinatory syndromes: past, present, and future. Dialogues Clin Neurosci 9(2):173-189.
- Holroyd S. Rabins PV (1996) A Three-Year Follow-Up Study of Visual Hallucinations in Patients with Macular Degeneration. J Nerv Ment Dis 184(3):188-189.
- Madill SA, Ffytche DH (2005) Charles Bonnet syndrome in patients with glaucoma and good acuity. Br J Ophthalmol 89(6): 785-786.
- Ffytche DH, Howard RJ, Brammer MJ, David A, Woodruff P, et al. (1998) The anatomy of conscious vision: an fMRI study of visual hallucinations. Nat. Neurosci 1(8): 738-742.
- Pliskin NH, Kiolbasa TA, Towle VL, Pankow L, Ernest JT, et al. (1996) Charles Bonnet Syndrome: An Early Marker for Dementia? J Am Geriatr Soc 44 (9): 1055-1061.
- Santhouse AM, Howard RJ, Ffytche DH (2000) Visual hallucinatory syndromes and the anatomy of the visual brain. Brain 123(10): 2055-2064.
- Manford M, Andermann F (1998) Complex visual hallucinations: Clinical and neurobiological insights. Brain 121(10): 1819-1840.
- Biousse V, Skibell BC, Watts RL, Loupe DN, Drews-Botsch C, et al. (2004) Ophthalmologic features of Parkinson’s disease. Neurology 62 (2): 177-180.
- Mocellin R, Walterfang M, Velakoulis D (2006) Neuropsychiatry of complex visual hallucinations. Aust N Z J Psychiatry 40(9): 742-751.
- Kazui H, Ishii R, Toshida T, Ikezawa J, Takaya M, et al. (2009) Neuroimaging studies in patients with Charles Bonnet Syndrome. Psychogeriatrics 9(2): 77-84.
- Adamczyk DT (1996) Visual phenomena, disturbances, and hallucinations. Optom Clin 5(3-4): 33-52.
- Bartlett JD, Jaanus SD (2008) Clinical Ocular Pharmacology. (5th edtn), St.Louis:Butterworth-Heinemann.
- Tomsak RL, Zaret CR, Weidenthal D (2003) Charles Bonnet syndrome precipitated by brimonidine tartrate eye drops. Br J Ophthalmol 87(7):917.
- Rahman I, Fernando B, Harrison M (2003) Charles Bonnet syndrome and brimonidine: comments. Br J Ophthalmol 88(5): 724.
- Haddad PM, Benbow SM (1992) Visual Hallucinations as the Presenting Symptom of Senile Dementia. Br J Psychiatry 161:263-265.
- Guerra-Garcia H (1997) Charles Bonnet Syndrome and Early Dementia. J Am Geriatr Soc 45(7):893-894.
- Alao AO, Hanrahan B (2003) Charles Bonnet Syndrome: Visual Hallucination and Multiple Sclerosis. Int J Psychiatry Med 33(2): 195-199.
- Lang UE, Stogowski D, Schulze D, Domula M, Schmidt E, et al. (2007) Charles Bonnet Syndrome: successful treatment of visual hallucinations due to vision loss with selective serotonin reuptake inhibitors. J Psychopharmacol 21(5): 553-555.
- Terao T (2000) Hallucinations in Alzheimer’s Disease and Charles Bonnet Syndrome. Am J Psychiatry 157(12):2062.
- Mahgoub N, Serby M (2007) Charles Bonnet Syndrome: Long-term Outcome of Treatment. Psychiatric Annals 37(8):579-580.
- Jackson ML, Ferencz J (2009) Charles Bonnet syndrome: visual loss and hallucinations. CMAJ 181(3-4):175-176.
- Garcia-Catalan MR, Arriola-Villalobos P, Santos-Bueso E, Gil-de-Bernable J, Diaz-Valle D, et al. (2013) Charles Bonnet syndrome precipitated by brimonidine. Arch Soc Esp Oftalmol 88(9):362-364.
- Yacoub R, Ferrucci S (2011) Charles Bonnet syndrome. Optometry 82:421-427.
- Hartney KE, Catalano G, Catalano M (2011) Charles Bonnet Syndrome: Are Medications Necessary? J Psychiatr Pract 17(2):137-141.
- Hughes DF (2013) Charles Bonnet syndrome: a literature review into diagnostic criteria, treatment and implications for nursing practice. J Psychiatr Ment Health Nurs 20:169-175.
- Gilmour G, Schreiber C, Ewing C (2009) An examination of the relationship between low vision and Charles Bonnet syndrome. Can J Ophthalmol 44:49-52.
- Vale TC, Fernandes LC, Caramelli P (2014) Charles Bonnet syndrome: characteristics of its visual hallucinations and differential diagnosis. Arq Neuropsiquiatr 72(5):333-336.





