Central Odontogenic Fibroma: Collection of Cases in the World Literature.
Case Report with use of Adjuvant Treatment for the Reduction of Recurrence with Liquid Nitrogen and Bone Regeneration
Guided with Lyophilized Bone and Platelet-Rich Plasma
García-Cano E1*, González-Magaña F2, Malagón-Hidalgo HO3, Caicedo-Perez JH1, Carrillo-Ponce CS4, Montiel-Jarquín AJ5
1 Plastic and Reconstructive Surgery Resident. Medical Center ISSEMYM, Toluca, México.
2 Maxillofacial Attending physician. Medical Center ISSEMYM, Toluca, México.
3 Head department of Plastic, Reconstructive and Maxillofacial Surgery. Medical Center ISSEMYM, Toluca, México.
4 Pathologist Attending physician. Medical Center ISSEMYM, Toluca, México.
5 Head department of education, High Specialty Medical Unit, IMSS, Puebla, México.
*Corresponding Author
García-Cano Eugenio,
Avenida Baja Velocidad 284, Metepec, Estado de México, México. P.C. 52170, USA.
Tel: +52 222 2602358
E-mail: eugenio_g_c@hotmail.com
Received:May 09, 2016; Accepted: June 06, 2016; Published: June 07, 2016
Citation: García-Cano E, et al., (2016) Central Odontogenic Fibroma: Collection of Cases in the World Literature. Case Report with use of Adjuvant Treatment for the Reduction of Recurrence with Liquid Nitrogen and Bone Regeneration Guided with Lyophilized Bone and Platelet-Rich Plasma. Int J Dentistry Oral Sci. S3:002, 11-15.DOI : dx.doi.org/10.19070/2377-8075-SI03002
Copyright: García-Cano E© 2016. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Abstract
Objective: The central odontogenic fibroma is an extremely rare neoplasm found in 0.1% of all odontogenic tumors. Mosqueda-Taylor et al, described 92 cases in the literature until 2011.
Study desining: 15 years old female, with increased volume in the right mandibular body region. The histopathological result a central odontogenic fibroma. The patient underwent enucleation and curettage, we applied liquid nitrogen on the surgical bed and cadaveric cancellous bone with platelel-rich plasma in the deffect secondary to the procedure. Using the search engines EBSCO and SCOPUS, all reports with histopathological confirmation of central odontogenic fibroma were included.
Results: No recurrence in our case was reported after twelve months follow-up. We found 121 reported cases in the english
literature including ours.
Conclusion: It is an extremely rare tumor. The use of liquid nitrogen, lyophilized bone and platelet-rich plasma as adjuvants methods to lower the reported recurrence and accelerate the bone healing process are feasible.
2.Case Report
3.Discussion
4.Conclusion
5.References
Introduction
The central odontogenic fibroma (COF) is an extremely rare benign neoplasm of intraosseous or central presentation found in only 0.1% of all odontogenic tumors [1,2]. It is considered histologically among the odontogenic tumors of mesenchymal tissue, with or without formation of odontogenic epithelium [1]. The World Health Organization (WHO) defines it as a benign proliferation of ectomesenchyme fibroblastic tissue characterized by a variable number of apparently inactive odontogenic epithelium [3]. There are two distinct histological types; 1. Simple COF, which presents as a poorly cellular and myxoid fibroblastic neoplasia without odontogenic epithelial component. 2. WHO or complex COF, with abundant odontogenic epithelium cell with foci of calcification [4].
Radiologically, the COF tends to be a well-defined lesion, radio lucid, uni or multilocular. In rare cases it can present as a mixed radio lucid lesion and present radiopaque characteristics with poorly defined borders [5-7].
Clinically, it presents as an asymptomatic slow-growing tumor, which in many cases remain undetected until the appearance of edema. It presents more frequently in females in a range of 2.8:1. They appear in both the maxilla and mandible (55% and 45% respectively). (2.4) In the maxilla it tends to include the anterior area, while in the jaw it presents most often in the molar and premolar region [2].
Mosqueda-Taylor et al, described 92 cases in the literature until 2011 [9] from that starting point, we decided to make a collection of the cases reported in the English-language literature, to know the current number of reported cases. We present the management of this rare entity, with a conservative surgical management, focused on early bone regeneration and use of adyuvant to minimize local recurrence.
Case Report
Female of 15 years old, who perceived increased volume in the right mandibular body region, four months after its appearance she was sent to our department. The lesion increases progressively to a clear distortion of the right mandibular body, being asymptomatic (Figure 1). In the physical examination, we observed increased intra oral volume at level of the first and second inferior right molars, without tenderness (Figure 2). In the orthopantomography a lesion, with regular borders, unilocular, radio lucid, with proximity to the lower right third unerupted molar, is observed; it also shifts medially adjacent teeth to the lesion (Figure 3). The facial computerized axial tomography scan, demonstrates a well-defined lesion, with regular borders, confined to the right mandibular body, causing bicortical expansion, being close to the right lower third molar unerupted (Figure 4).
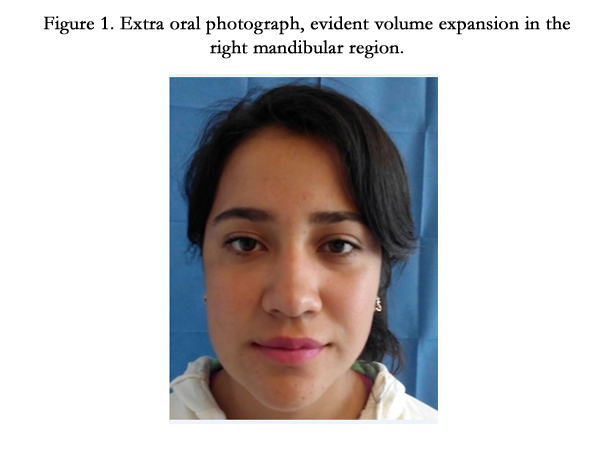

Figure 1. Extra oral photograph, evident volume expansion in the right mandibular region.
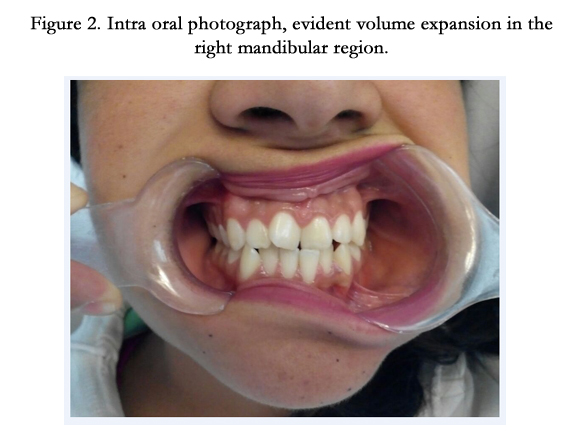

Figure 2. Intra oral photograph, evident volume expansion in the right mandibular region.
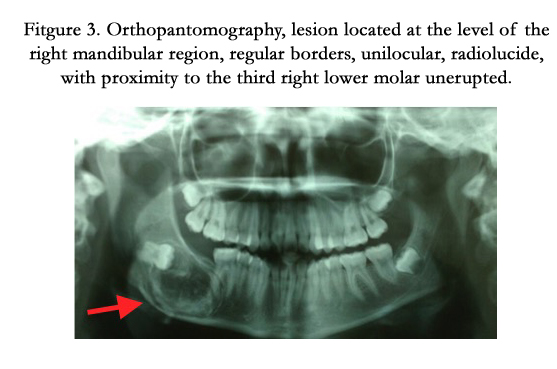
Fitgure 3. Orthopantomography, lesion located at the level of the right mandibular region, regular borders, unilocular, radiolucide, with proximity to the third right lower molar unerupted.
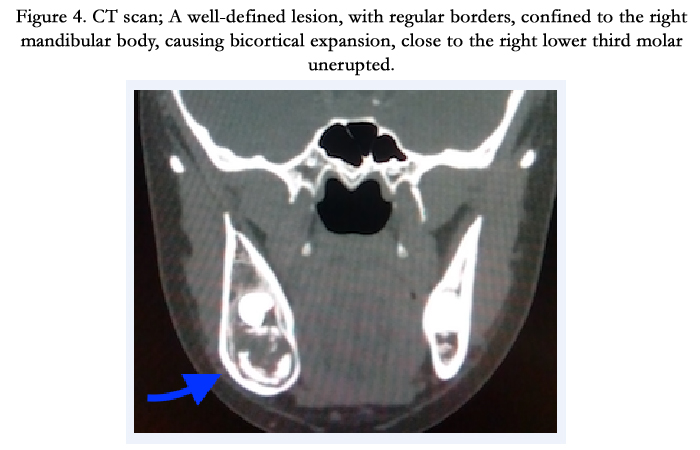
Figure 4. CT scan; A well-defined lesion, with regular borders, confined to the right mandibular body, causing bicortical expansion, close to the right lower third molar unerupted.
The patient was scheduled for enucleation and curettage of the lesion. The procedure was performed through a vestibular incision of 5cm over the right mandibular body, periosteum and oral corticotomy was done, allowing full exposure of the lesion and unenrupted molar (Figure 5). A complete enucleation of the lesion was achieved and we performed curettage and complete extraction of the third unerupted molar (Figura 6). Liquid nitrogen on the surgical bed was applied, ensuring not to injure the alveolar nerve which was protected by gel foam (Figure 7). Afterwards cadaveric cancellous bone was placed followed by application of platelet-rich plasma to fill the defect (Figure 8), proceding to seal the oral mucosa with absorbable suture.
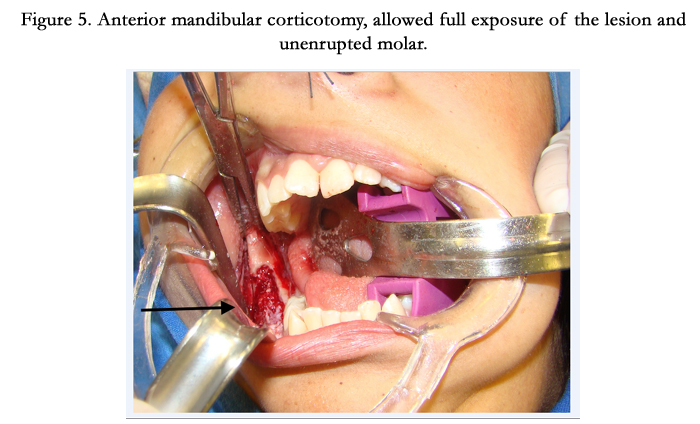
Figure 5. Anterior mandibular corticotomy, allowed full exposure of the lesion and unenrupted molar.
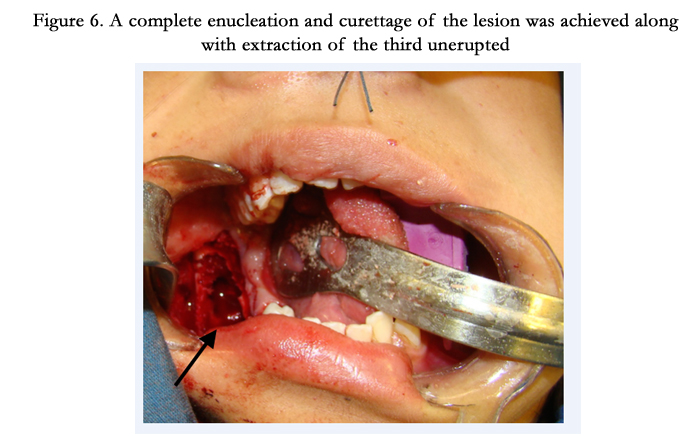
Figure 6. A complete enucleation and curettage of the lesion was achieved along with extraction of the third unerupted molar.
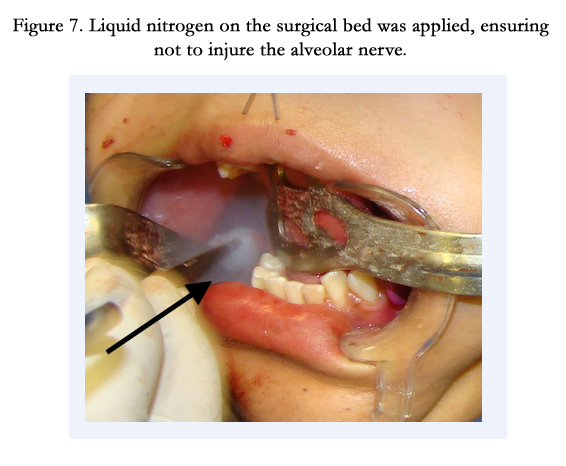
Figure 7. Liquid nitrogen on the surgical bed was applied, ensuring not to injure the alveolar nerve.
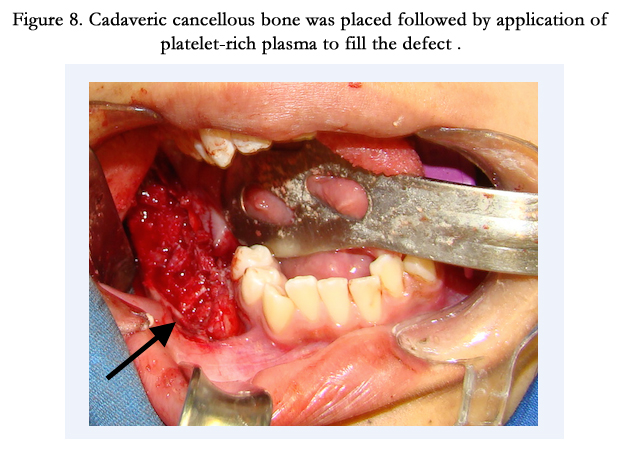
Figure 8. Cadaveric cancellous bone was placed followed by application of platelet-rich plasma to fill the defect .
In the microscopic review with conventional hematoxylin-eosin was identified a mesenchymal lesion with a growth pattern in solid mantles comprised of acellular eosinophilic material with focal and isolated odontogenic epithelium with cores which retain their polarity, without nucleoli, mitosis, cytologic atypia or calcifications. These characteristics corresponding to a simple type injury according to the WHO classification. (Figura 9).
Twelve months after the surgical procedure the extra oral mandibular right bulking shows no progression (Figure 10). The post operative control was carried out with clinical and radiographic examination. In the intra oral examination the surgical scar showed no evidence of recurrence of injury at this level. In the control orthopantomography no recurrence is observed, with obvious bone regeneration (Figure 11).
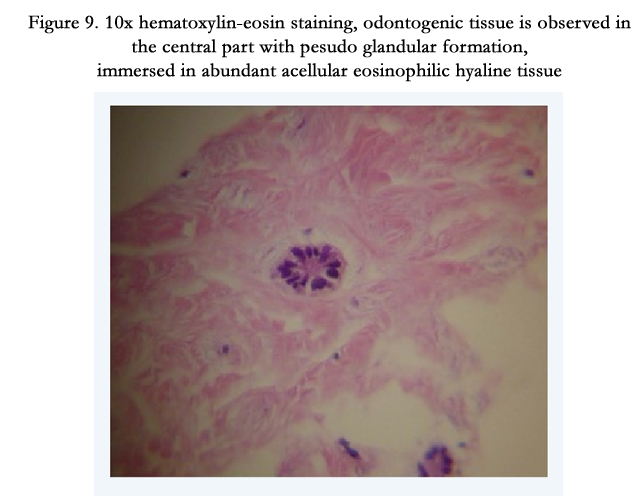
Figure 9. 10x hematoxylin-eosin staining, odontogenic tissue is observed in the central part with pesudo glandular formation, immersed in abundant acellular eosinophilic hyaline tissue

Figure 10. Twelve months after the surgical procedure the extra oral mandibular right bulking shows no progression.
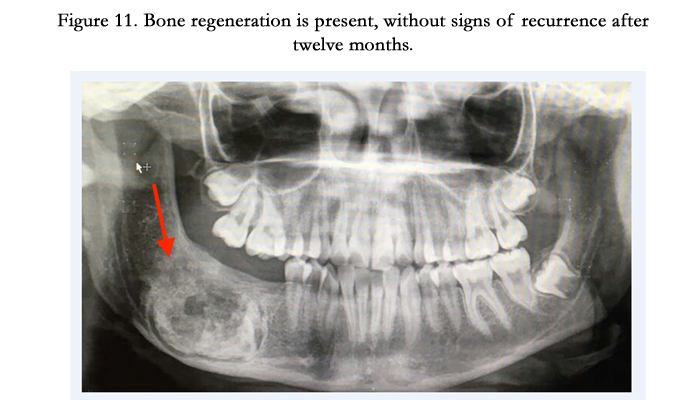
Figure 11. Bone regeneration is present, without signs of recurrence after twelve months.
Discussion
The central odontogenic fibroma is one of the rarest and least understood odontogenic neoplasms, according to the literature corresponds to only 0.1% of all odontogenic tumors [1,2]. In the literature few cases have been reported. The last review in 2011 by Mosqueda-Taylor et al [9], described 92 cases worldwide. Using the search engines EBSCO and SCOPUS, all the case reports with histopathological confirmation of central odontogenic fibroma were identified and included. We found 121 reported cases in the english-speaking language in the world literature including ours [2,8,9,10-28].
Being an extremely rare entity it does not have clinical treatment guidelines, so it is essential to take into account the experience reported in the literature, as well as their success.
In the series of 92 cases reported by Taylor et al, aproximately 55% involved the mandible, the range age reported by Taylor et al is from 4 to 80 years and most cases are diagnosed during the second to fourth decades of life. The reported incidence of an unerupted tooth is 27% [9].
The revision made by Ramet et al., [3], show a predilection for female sex in a 69%, while the incidence in our revision shows a predilection for male sex in a 62% (18 of 29 patients).
The first authors who reported curettage as first-line treatment were Dunlap and Barker, who presented two cases of maxillary odontogenic fibroma treated by this method with a follow-up of 9 and 10 years without evidence of recurrence [29].
There is no a revision for the time of follow-up after treatment for this tumor. Therefore, we decided to made a revision on this topic. Out of the 29 patients, 23 were treated by enucleation and curettage (2 were treated the same way, but did not have a follow-up information) with a mean follow up of 20.73 months without any evidence of recurrence; 2 were treated by segmentary resection with a mean follow-up of 18 months, without evidence of recurrence; and 2 were treated by resection in bloc, without evidence of recurrence. The primary treatment is enucleation and curettage which has proved to be an effective treatment with no evidence of recurrence in a medium term [1-22,24-28].
In our attempt to reduce the low risk of recurrence, the use of liquid nitrogen (NL) has been described for treatment of some bone tumors. The NL causes the formation of intracellular ice crystals, resulting in a membrane disruption and consequently induce cell necrosis. It has been proven effective as an adjuvant action in curettage for a variety of benign and malignant bone tumors of low grade, which is why we decided to use it in this procedure [30].
The effect caused by the tumor enucleation and curettage, entails a normal course of bone regeneration, there is no experience reported on the use of lyophilized bone in these type of tumors; however, there is a report by Bahadir et al, in which mentions its use to rebuild the cavity caused by the complete enucleation of odontogenic giant cystic lesions in 17 patients. Bone regeneration with lyophilized bone showed strong acumulative effect with a faster bone healing process [31]. This effect was shown in the orthopantomography control three months after surgery, in which an accelerated bone healing process was demonstrated.
Platelet rich plasma is a concentration of platelets in blood plasma, its active form contains derived growth factor containing platelets (PDGF), Factor-β (TGF-β) Vascular Endothelial Growth factor (VEGF), the growth factor epidermal (EGF), fibroblast growth factor (FGF), and a number of macrophages and monocytes mediators of a variety of cytokines capable of mediating inflammation. The use of this therapy has regenerative advantages in bone healing accelerating the process [32], for this reason we decided the application of platelet rich plasma in the cavity secondary to complete enucleation of the lesion, together with with lyophilized bone.
All these adjuvant treatments theoretically promotes a lower risk of recurrence and faster bone healing.
Conclusion
The Central Odontogenic Fibroma is an extremely rare tumor; only 121 cases are reported worldwide in the English literature. Surgical treatment of first instance should be conservative with complete enucleation and curettage of the surgical bed. The use of liquid nitrogen can be an effective adyuvant to prevent recurrence of the lesion. In our experience lyophilized bone in conjunction with platelet-rich plasma is feasible to accelerate the process of bone healing.
References
- Muñóz-Torres C, Reyes- Olave P, Álvarez-Novoa C, Venegas-Rojas B (2010) Fibroma odontogénico central, tipo WHO: Reporte de un caso y revisión de la literatura. REV ESP CIR ORAL MAXILOFAC 32(4): 159-164.
- Salgado H, Mesquita P (2014) Central odontogenic fibroma of the maxilla – A case report. REV PORT ESTOMATOL MED DENT CIR MAXILOFAC 55(1): 49-54.
- Cortés-Castillo G, Liceaga-Reyes R, Mosqueda-Taylor A (2011) Lesión mandibular inusual de fibroma odontogénico central combinado con granuloma central de células gigantes mandibular. Rev Odont Mex 15(2): 126-131.
- Pushpanshu K, Kaushik R, Punyani SR, Jasuja V, Raj V, Seshadri A (2013) Concurrent central odontogenic fibroma (WHO Type) and traumatic bone cyst: report of a rare case. Quant Imaging Med Surg 3(6): 341-346.
- Han-Ping C, Lo-Lin T (2008) Central Odontogenic Fibroma of Mandible – A Case Report. Taiwan J Oral Maxillofac Surg 19: 179-185.
- Daskala I, Kalyvas D, Kolokoudias M, Vlachodimitropoulos D, Alexandridis C (2009) Central odontogenic fibroma of the mandible: a case report. Journal of Oral Science 51(3): 457-461.
- Thankappan P, Chundru NSV, Amudala R, Yanadi P, Rahamthullah SAKU, Botu M (2014) Central Odontogenic Fibroma of Simple Type. Case reports in dentistry.
- Matos FR, Moraes M, Neto AC, Miguel Mc, da Silveira EJ (2011) Central Odontogenic Fibroma. Ann Diagn Pathol 15(6): 481-484.
- Mosqueda-Taylor A, Martínez-Mata G, Carlos-Bregni R, Agustin-Vargas P, Toral-Rizo V, Cano-Valdéz AM, et al. (2011) Central odontogenic fibroma: new findings and report of a multicentric collaborative study. Pathol Oral Radiol Endod 112(3): 349-358.
- Hrichi R, Gargallo-Albiol J, Berini-Ayés L, Gay-Escoda C (2012) Central odontogenic fibroma:retrospective study of 8 clinical cases. Med Oral Patol Oral Cir Bucal 17(1): e50-55.
- Anbiaee N, Ebrahimnejad H, Sanaei A (2015) Central odontogenic fibroma (simple type) in a four-year-old boy: atypical cone-beam computed tomographic appearance with periosteal reaction. Imaging Sci Dent 45(2): 109-115.
- Singh HP, Indra BN, Giri KY, Dandriyal R, Mall SL (2014) Central Odontogenic Fibroma of the Mandible. J Dent Sci Oral Rehab 5(3): 165-167.
- Nah KS (2011) Central odontogenic fibroma: a case report. Imaging Sci Dent 41(2): 85-88.
- Takeoka T, Inui M, Okumura K, Nakamura S, Shimizu K, Tagawa T (2013) A central odontogenic fibroma mimicking a dentigerous cyst associated with an impacted mandibular third molar – Immunohisological study and review of literature. Journal of Oral and Maxillofacial Surgery, Medicine, and Pathology 25(2): 193-196.
- Gopinathan PA, Kokila G, Jyothi M, Nair MS, Jacob TV, Praveen KS (2014) Importance of Histopathology in Diagnosis of Central Odontogenic Fibroma – A Case Report. Research Journal of Pharmaceutical, Biological and Chemical Sciences 5(6): 923-928.
- Shirashi T, Uehara M, Fujita S, Ikeda T, Asahina I (2015) A case of central odontogenic fibroma in a pediatric patient: Mandibular reconstruction with parietal bone. Journal of Oral Maxillofacial Surgery, Medicine and Pathology 27(3): 361-365.
- Hara M, Matsuzaki H, Katase N, Yanagi Y, Unetsubo T, Asaumi J, et al. (2012) Central odontogenic fibroma of the jawbone: 2 case reports describing its imaging features and an analysis of its DCE-MRI findings. Oral Surg Oral Med Oral Pathol Oral Radiol 113(6): e51-58.
- Batson JP, Strickland F (2014) Central Odontogenic Fibroma: Case Report and Review. US Army Med Dep J 57-60.
- Soolari A, Khan A (2014) Central Odontogenic Fibroma of the Gingiva: A Case Report. Open Dent J 8: 280-288.
- Veeravarmal V, Nirmal-Madhavan R, Mohamed-Nassar M, Amsaveni R (2013) Central odontogenic fibroma of the maxilla. J Oral Maxillofac Pathol 17(2): 319.
- Venugopal S, Radhakrishna S, Raj A, Sawhney A (2014) Central odontogenic fibroma. J Indian Soc Periodontol 18(2): 240-243.
- Schussel JL, Gallottini MHC, Braz-Silva PH (2014) Odontogenic fibroma WHO-type simulating periodontal disease: Report of a case. J Indian Soc Periodontol18(1): 85-87.
- Kimura T, Ohba S, Yoshimura H, Katase N, Imamura Y, Ueno T, et al. (2013) Epithelium-poor type Central Odontogenic Fibroma: An immunohistological Study and Review of the Literature. Journal of Hard Tissue Biology 22(2): 273-278.
- Niklander S, Martínez R, Deichler J, Esguep A (2011) Bilateral mandibular odontogenic fibroma (WHO type): Report of a case with 5-year radiographic follow-up. JOURNAL OF DENTAL SCIENCES 6(2): 123-127.
- Salehinejad J, Ghazi N, Heravi FB, Ghazi E (2015) Concurrent central odontogenic fibroma (WHO type) and odontoma: Report of a rare and unusual entity. Journal of Oral and Maxillofacial Surgery, Medicine and Pathology 27(6): 888-892. DOI: 10.1016/j.ajoms.2015.04.002
- Molina RN, Ruiz LP, Taylor AM, Ramírez HGH, Lonato JAP, Gónzalez- Gónzalez R (2011) Central odontogenic fibroma combined with central giant cell lesión of the mandible. Immunohistochemical profile. J Clin Exp Dent 3(4): 348-351.
- Ahmadi SK, Rahpeyma A (2012) Central Odontogenic Fibroma of the Mandible. J Dent Mater Tech 1(2): 70-73.
- Iordanidis S, Poulopoulos A, Epivatianos A, Zouloumis L (2013) Central odontogenic fibroma: report of case qith immunohistochemical study. Indian J Dent Res 24(6): 753-755.
- Dunlap C, Barker B (1984) Central odontogenic fibroma of the WHO type. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 57(4): 390-394.
- Bickels J, Meller I, Shmookler BM, Malawer MM (1999) The role and biology of Cryosurgery in the treatment of Bone Tumors: A review. Acta Orthop Scand 70(3): 308-315.
- Bahadir G, Gokce M (2007) Allogenic Grafts in Oral Surgery: Clinical Findings and Follow-up. Hacettepe Dishekimligi Fakultesi Dergisi 31(2): 31-37.
- Rodriguez IA, Growney-Kalaf EA, Bowlin GL, Sell SA (2014) Platelet-Rich Plasma in Bone Regeneration: Engineering the Delivery for Improved Clinical Efficacy. BioMed Research International.





